{"title":"刺缝线引起腹腔镜骶骶固定术后急性小肠阻塞。","authors":"Dipak Limbachiya, Rajnish Tiwari, Rashmi Kumari, Manoj Aggarwal","doi":"10.4293/CRSLS.2022.00058","DOIUrl":null,"url":null,"abstract":"Introduction: A case report of small bowel obstruction related to barbed suture in a postoperative patient of laparoscopic sacrocolpopexy. Case Description: A 61 -year-old female with a body mass index of 27 with vault prolapse underwent laparoscopic sacrocolpopexy. The patient was discharged on postoperative day two. She presented again in the emergency department on the fifth postoperative day with complaints of frequent vomiting episodes with intermittent and colicky pain in the abdomen. Her imaging (computed tomography abdomen/pelvis with oral contrast) suggested distal small bowel mechanical obstruction at midileum with significant free fluid in the peritoneum. Emergency laparoscopic exploration was done. Peroperative V-LocTM 180 suture tail end barbs were found anchored to the mesentery of midileum causing a loop that led to compression and occlusion of distal bowel. The barbed suture tail end was detached from the mesentery and thus relieving the compression. No additional procedure was required for the bowel wall. The excess barbed suture tail end outside the peritoneum was trimmed. The postoperative course was uneventful. Conclusion: Bowel complication is an uncommon but serious issue following the use of barbed sutures. It should be used with utmost caution as none of the preventive measures are completely safe. Further studies need to be done for preventive measures.","PeriodicalId":72723,"journal":{"name":"CRSLS : MIS case reports from SLS","volume":"9 4","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/e6/e2022.00058.PMC9682608.pdf","citationCount":"1","resultStr":"{\"title\":\"Barbed Suture Causing Acute Small Bowel Obstruction Post Laparoscopic Sacrocolpopexy.\",\"authors\":\"Dipak Limbachiya, Rajnish Tiwari, Rashmi Kumari, Manoj Aggarwal\",\"doi\":\"10.4293/CRSLS.2022.00058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Introduction: A case report of small bowel obstruction related to barbed suture in a postoperative patient of laparoscopic sacrocolpopexy. Case Description: A 61 -year-old female with a body mass index of 27 with vault prolapse underwent laparoscopic sacrocolpopexy. The patient was discharged on postoperative day two. She presented again in the emergency department on the fifth postoperative day with complaints of frequent vomiting episodes with intermittent and colicky pain in the abdomen. Her imaging (computed tomography abdomen/pelvis with oral contrast) suggested distal small bowel mechanical obstruction at midileum with significant free fluid in the peritoneum. Emergency laparoscopic exploration was done. Peroperative V-LocTM 180 suture tail end barbs were found anchored to the mesentery of midileum causing a loop that led to compression and occlusion of distal bowel. The barbed suture tail end was detached from the mesentery and thus relieving the compression. No additional procedure was required for the bowel wall. The excess barbed suture tail end outside the peritoneum was trimmed. The postoperative course was uneventful. Conclusion: Bowel complication is an uncommon but serious issue following the use of barbed sutures. It should be used with utmost caution as none of the preventive measures are completely safe. Further studies need to be done for preventive measures.\",\"PeriodicalId\":72723,\"journal\":{\"name\":\"CRSLS : MIS case reports from SLS\",\"volume\":\"9 4\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/e6/e2022.00058.PMC9682608.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CRSLS : MIS case reports from SLS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4293/CRSLS.2022.00058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CRSLS : MIS case reports from SLS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4293/CRSLS.2022.00058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Barbed Suture Causing Acute Small Bowel Obstruction Post Laparoscopic Sacrocolpopexy.
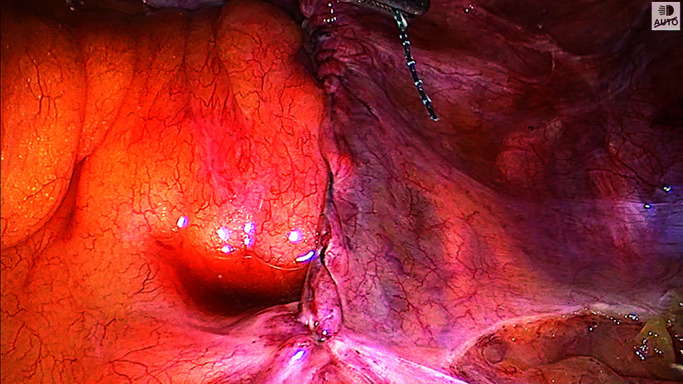
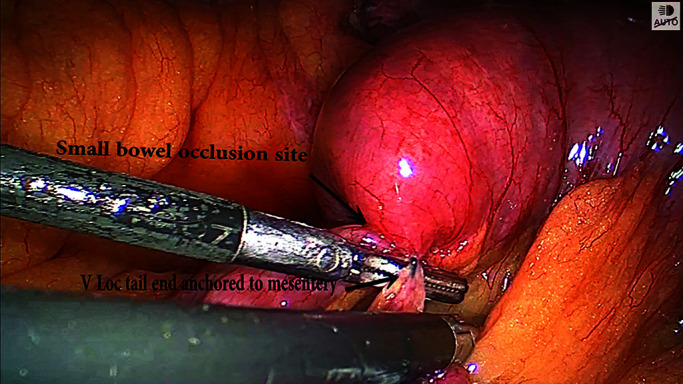
Introduction: A case report of small bowel obstruction related to barbed suture in a postoperative patient of laparoscopic sacrocolpopexy. Case Description: A 61 -year-old female with a body mass index of 27 with vault prolapse underwent laparoscopic sacrocolpopexy. The patient was discharged on postoperative day two. She presented again in the emergency department on the fifth postoperative day with complaints of frequent vomiting episodes with intermittent and colicky pain in the abdomen. Her imaging (computed tomography abdomen/pelvis with oral contrast) suggested distal small bowel mechanical obstruction at midileum with significant free fluid in the peritoneum. Emergency laparoscopic exploration was done. Peroperative V-LocTM 180 suture tail end barbs were found anchored to the mesentery of midileum causing a loop that led to compression and occlusion of distal bowel. The barbed suture tail end was detached from the mesentery and thus relieving the compression. No additional procedure was required for the bowel wall. The excess barbed suture tail end outside the peritoneum was trimmed. The postoperative course was uneventful. Conclusion: Bowel complication is an uncommon but serious issue following the use of barbed sutures. It should be used with utmost caution as none of the preventive measures are completely safe. Further studies need to be done for preventive measures.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


