{"title":"系统性硬化症中的普遍钙质沉着症。","authors":"Eaman Alhassan","doi":"10.1002/acr2.11527","DOIUrl":null,"url":null,"abstract":"The patient, a 46-year-old woman with a history of systemic sclerosis, interstitial lung disease, and dystrophic calcinosis cutis presented to the emergency department complaining of right thigh pain. Physical examination was notable for a large erythematous, tender, indurated circular area in the medial thigh with many large calci fi ed nodules throughout her thighs. Incision and drainage yielded a small amount of purulent chalky fl uid. The patient received antibiotics and was discharged home. Over 5 years, the patient had recurrent soft tissue infections with progressive calcinosis. Her basic metabolic panel was within normal limits (including calcium and phosphorus levels). Computed tomography showed extensive calci fi cation throughout the subcutaneous tissues of the pelvis and bilateral thighs. Some of the calcinosis extended into the intermuscular fascial planes of the adductor and posterior compartment musculature of the bilateral thighs. The patient received nifedipine, mycophenolic acid, rituximab, colchicine, and sodium thiosulfate (topical, intralesional, and intrave-nous), but her calcinosis continued to progress. Calcinosis is a debilitating condition that occurs in 40% of patients with systemic sclerosis. A long disease duration is associated with progressive calcinosis (1). Thus far, there are no effective treatment options for calcinosis.","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"5 3","pages":"105"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/b6/ACR2-5-105.PMC10010482.pdf","citationCount":"1","resultStr":"{\"title\":\"Calcinosis universalis in systemic sclerosis.\",\"authors\":\"Eaman Alhassan\",\"doi\":\"10.1002/acr2.11527\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"The patient, a 46-year-old woman with a history of systemic sclerosis, interstitial lung disease, and dystrophic calcinosis cutis presented to the emergency department complaining of right thigh pain. Physical examination was notable for a large erythematous, tender, indurated circular area in the medial thigh with many large calci fi ed nodules throughout her thighs. Incision and drainage yielded a small amount of purulent chalky fl uid. The patient received antibiotics and was discharged home. Over 5 years, the patient had recurrent soft tissue infections with progressive calcinosis. Her basic metabolic panel was within normal limits (including calcium and phosphorus levels). Computed tomography showed extensive calci fi cation throughout the subcutaneous tissues of the pelvis and bilateral thighs. Some of the calcinosis extended into the intermuscular fascial planes of the adductor and posterior compartment musculature of the bilateral thighs. The patient received nifedipine, mycophenolic acid, rituximab, colchicine, and sodium thiosulfate (topical, intralesional, and intrave-nous), but her calcinosis continued to progress. Calcinosis is a debilitating condition that occurs in 40% of patients with systemic sclerosis. A long disease duration is associated with progressive calcinosis (1). Thus far, there are no effective treatment options for calcinosis.\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\"5 3\",\"pages\":\"105\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/b6/ACR2-5-105.PMC10010482.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11527\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11527","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
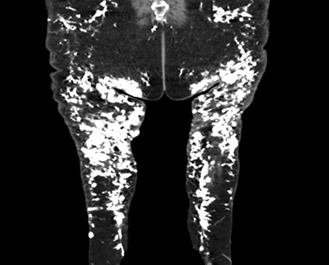
The patient, a 46-year-old woman with a history of systemic sclerosis, interstitial lung disease, and dystrophic calcinosis cutis presented to the emergency department complaining of right thigh pain. Physical examination was notable for a large erythematous, tender, indurated circular area in the medial thigh with many large calci fi ed nodules throughout her thighs. Incision and drainage yielded a small amount of purulent chalky fl uid. The patient received antibiotics and was discharged home. Over 5 years, the patient had recurrent soft tissue infections with progressive calcinosis. Her basic metabolic panel was within normal limits (including calcium and phosphorus levels). Computed tomography showed extensive calci fi cation throughout the subcutaneous tissues of the pelvis and bilateral thighs. Some of the calcinosis extended into the intermuscular fascial planes of the adductor and posterior compartment musculature of the bilateral thighs. The patient received nifedipine, mycophenolic acid, rituximab, colchicine, and sodium thiosulfate (topical, intralesional, and intrave-nous), but her calcinosis continued to progress. Calcinosis is a debilitating condition that occurs in 40% of patients with systemic sclerosis. A long disease duration is associated with progressive calcinosis (1). Thus far, there are no effective treatment options for calcinosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


