Khalid Halahleh, Rawan Mustafa, Dania Sarhan, Dalia Al Rimawi, Hadeel Abdelkhaleq, Isra Muradi, Iyad Sultan
{"title":"移植物CD3+ t细胞剂量对t细胞填充人白细胞抗原错配异体造血外周血干细胞移植结果的影响。","authors":"Khalid Halahleh, Rawan Mustafa, Dania Sarhan, Dalia Al Rimawi, Hadeel Abdelkhaleq, Isra Muradi, Iyad Sultan","doi":"10.14740/jh1071","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Data on whether the graft CD3-positive (CD3<sup>+</sup>) T-cell dose in T-cell-replete human leukocyte antigen (HLA)-mismatched allogeneic hematopoietic peripheral blood stem cells transplantation (PBSCT) influences post-transplant outcomes are controversial.</p><p><strong>Methods: </strong>Using King Hussein Cancer Center (KHCC) Blood and Marrow Transplantation (BMT) Registry database, 52 adult subjects, receiving the first T-cell-replete HLA-mismatched allogeneic hematopoietic PBSCT for acute leukemias or myelodysplastic syndrome, were identified, from January 2017 to December 2020. The cutoff value of graft CD3<sup>+</sup> T-cell dose was identified using the receiver operating characteristic (ROC) formula and Youden's analysis. Subjects were divided into two cohorts: cohort 1 with low CD3<sup>+</sup> T-cell dose (n = 34) and cohort 2 with high CD3<sup>+</sup> T-cell dose (n = 18). Correlative analyses were performed between CD3<sup>+</sup> T-cell dose and the risk of graft-versus-host disease (GvHD), relapse, relapse-free survival (RFS), and overall survival (OS). P-values were two-sided and considered significant when P < 0.05.</p><p><strong>Results: </strong>Subject covariates were displayed. Subject's characteristics were comparable, except for higher nucleated cells and more female donors in the high CD3<sup>+</sup> T-cell cohort. The 100-day cumulative incidence of acute GvHD (aGvHD) was 45±7% and 3-year cumulative incidence of chronic GvHD (cGvHD) was 28±6.7%. There was no statistically significant difference between the two cohorts in aGvHD (50% vs. 39%, P = 0.4) or cGvHD (29% vs. 22%, P = 0.7). The 2-year cumulative incidence of relapse (CIR) was 67.5±16.3% for low compared with 14.3±6.8% for high CD3<sup>+</sup> T-cell cohort (P = 0.018). Fifteen subjects relapsed and 24 have died, 13 due to disease relapse. There was an improvement in 2-year RFS (94% vs. 83%; P = 0.0022) and 2-year OS (91% vs. 89%; P = 0.025) in low CD3<sup>+</sup> T-cell cohort compared with high CD3<sup>+</sup> T-cell cohort. Graft CD3<sup>+</sup> T-cell dose is the only significant risk factor for relapse (P = 002), and OS (P = 0.030) in univariate analysis which was maintained in multivariate for relapse (P = 0.003), but not for OS (P = 0.050).</p><p><strong>Conclusions: </strong>Our data suggest that high graft CD3<sup>+</sup> T-cell dose is associated with lower risk of relapse, and might improve long-term survival, but has no influence on the risk of developing aGvHD or cGvHD.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"12 1","pages":"27-36"},"PeriodicalIF":1.3000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/29/jh-12-027.PMC9990716.pdf","citationCount":"0","resultStr":"{\"title\":\"The Impact of Graft CD3<sup>+</sup> T-Cell Dose on the Outcome of T-Cell Replete Human Leukocyte Antigen-Mismatched Allogeneic Hematopoietic Peripheral Blood Stem Cells Transplantation.\",\"authors\":\"Khalid Halahleh, Rawan Mustafa, Dania Sarhan, Dalia Al Rimawi, Hadeel Abdelkhaleq, Isra Muradi, Iyad Sultan\",\"doi\":\"10.14740/jh1071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Data on whether the graft CD3-positive (CD3<sup>+</sup>) T-cell dose in T-cell-replete human leukocyte antigen (HLA)-mismatched allogeneic hematopoietic peripheral blood stem cells transplantation (PBSCT) influences post-transplant outcomes are controversial.</p><p><strong>Methods: </strong>Using King Hussein Cancer Center (KHCC) Blood and Marrow Transplantation (BMT) Registry database, 52 adult subjects, receiving the first T-cell-replete HLA-mismatched allogeneic hematopoietic PBSCT for acute leukemias or myelodysplastic syndrome, were identified, from January 2017 to December 2020. The cutoff value of graft CD3<sup>+</sup> T-cell dose was identified using the receiver operating characteristic (ROC) formula and Youden's analysis. Subjects were divided into two cohorts: cohort 1 with low CD3<sup>+</sup> T-cell dose (n = 34) and cohort 2 with high CD3<sup>+</sup> T-cell dose (n = 18). Correlative analyses were performed between CD3<sup>+</sup> T-cell dose and the risk of graft-versus-host disease (GvHD), relapse, relapse-free survival (RFS), and overall survival (OS). P-values were two-sided and considered significant when P < 0.05.</p><p><strong>Results: </strong>Subject covariates were displayed. Subject's characteristics were comparable, except for higher nucleated cells and more female donors in the high CD3<sup>+</sup> T-cell cohort. The 100-day cumulative incidence of acute GvHD (aGvHD) was 45±7% and 3-year cumulative incidence of chronic GvHD (cGvHD) was 28±6.7%. There was no statistically significant difference between the two cohorts in aGvHD (50% vs. 39%, P = 0.4) or cGvHD (29% vs. 22%, P = 0.7). The 2-year cumulative incidence of relapse (CIR) was 67.5±16.3% for low compared with 14.3±6.8% for high CD3<sup>+</sup> T-cell cohort (P = 0.018). Fifteen subjects relapsed and 24 have died, 13 due to disease relapse. There was an improvement in 2-year RFS (94% vs. 83%; P = 0.0022) and 2-year OS (91% vs. 89%; P = 0.025) in low CD3<sup>+</sup> T-cell cohort compared with high CD3<sup>+</sup> T-cell cohort. Graft CD3<sup>+</sup> T-cell dose is the only significant risk factor for relapse (P = 002), and OS (P = 0.030) in univariate analysis which was maintained in multivariate for relapse (P = 0.003), but not for OS (P = 0.050).</p><p><strong>Conclusions: </strong>Our data suggest that high graft CD3<sup>+</sup> T-cell dose is associated with lower risk of relapse, and might improve long-term survival, but has no influence on the risk of developing aGvHD or cGvHD.</p>\",\"PeriodicalId\":15964,\"journal\":{\"name\":\"Journal of hematology\",\"volume\":\"12 1\",\"pages\":\"27-36\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/29/jh-12-027.PMC9990716.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jh1071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
The Impact of Graft CD3+ T-Cell Dose on the Outcome of T-Cell Replete Human Leukocyte Antigen-Mismatched Allogeneic Hematopoietic Peripheral Blood Stem Cells Transplantation.
Background: Data on whether the graft CD3-positive (CD3+) T-cell dose in T-cell-replete human leukocyte antigen (HLA)-mismatched allogeneic hematopoietic peripheral blood stem cells transplantation (PBSCT) influences post-transplant outcomes are controversial.
Methods: Using King Hussein Cancer Center (KHCC) Blood and Marrow Transplantation (BMT) Registry database, 52 adult subjects, receiving the first T-cell-replete HLA-mismatched allogeneic hematopoietic PBSCT for acute leukemias or myelodysplastic syndrome, were identified, from January 2017 to December 2020. The cutoff value of graft CD3+ T-cell dose was identified using the receiver operating characteristic (ROC) formula and Youden's analysis. Subjects were divided into two cohorts: cohort 1 with low CD3+ T-cell dose (n = 34) and cohort 2 with high CD3+ T-cell dose (n = 18). Correlative analyses were performed between CD3+ T-cell dose and the risk of graft-versus-host disease (GvHD), relapse, relapse-free survival (RFS), and overall survival (OS). P-values were two-sided and considered significant when P < 0.05.
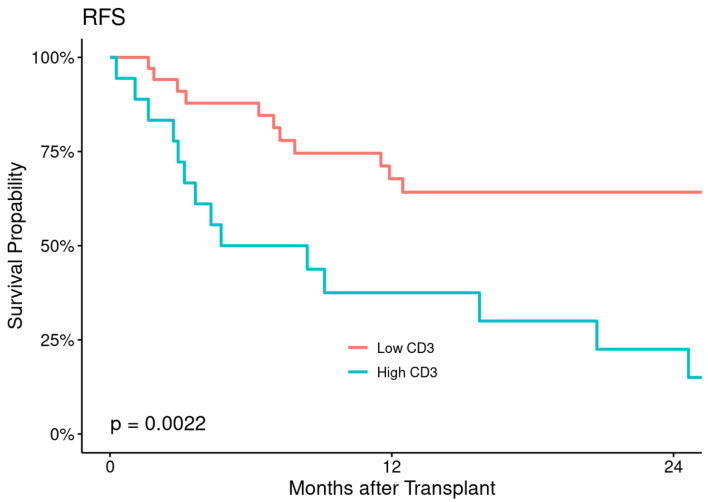
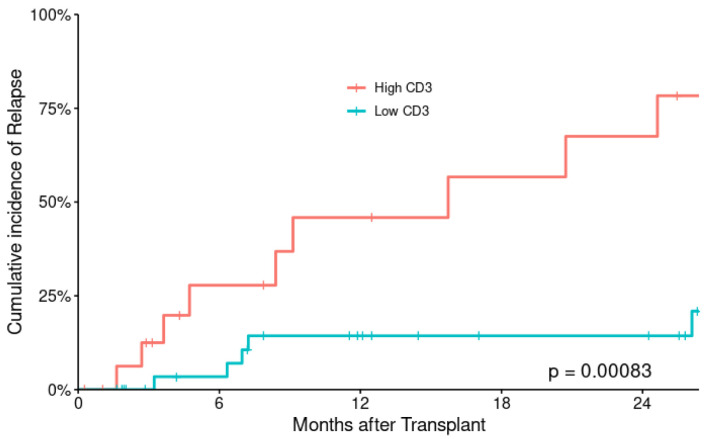
Results: Subject covariates were displayed. Subject's characteristics were comparable, except for higher nucleated cells and more female donors in the high CD3+ T-cell cohort. The 100-day cumulative incidence of acute GvHD (aGvHD) was 45±7% and 3-year cumulative incidence of chronic GvHD (cGvHD) was 28±6.7%. There was no statistically significant difference between the two cohorts in aGvHD (50% vs. 39%, P = 0.4) or cGvHD (29% vs. 22%, P = 0.7). The 2-year cumulative incidence of relapse (CIR) was 67.5±16.3% for low compared with 14.3±6.8% for high CD3+ T-cell cohort (P = 0.018). Fifteen subjects relapsed and 24 have died, 13 due to disease relapse. There was an improvement in 2-year RFS (94% vs. 83%; P = 0.0022) and 2-year OS (91% vs. 89%; P = 0.025) in low CD3+ T-cell cohort compared with high CD3+ T-cell cohort. Graft CD3+ T-cell dose is the only significant risk factor for relapse (P = 002), and OS (P = 0.030) in univariate analysis which was maintained in multivariate for relapse (P = 0.003), but not for OS (P = 0.050).
Conclusions: Our data suggest that high graft CD3+ T-cell dose is associated with lower risk of relapse, and might improve long-term survival, but has no influence on the risk of developing aGvHD or cGvHD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


