Prateek Sharma, Gary W Falk, Menaka Bhor, A Burak Ozbay, Dominick Latremouille-Viau, Annie Guerin, Sherry Shi, Margaret M Elvekrog, Paul Limburg
{"title":"美国胃食管反流病、巴雷特食管和巴雷特食管相关肿瘤患者的医疗资源利用和成本。","authors":"Prateek Sharma, Gary W Falk, Menaka Bhor, A Burak Ozbay, Dominick Latremouille-Viau, Annie Guerin, Sherry Shi, Margaret M Elvekrog, Paul Limburg","doi":"10.36469/001c.68191","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Gastroesophageal reflux disease (GERD) is a risk factor for Barrett's esophagus (BE) and BE-related neoplasia (BERN). <b>Objectives:</b> This study aimed to evaluate healthcare resource utilization (HRU) and costs associated with GERD, BE, and BERN in the United States. <b>Methods:</b> Adult patients with GERD, nondysplastic BE (NDBE), and BERN (including indefinite for dysplasia [IND], low-grade dysplasia [LGD], high-grade dysplasia [HGD] or esophageal adenocarcinoma [EAC]), were identified from a large US administrative claims database, the IBM Truven Health MarketScan® databases (Q1/2015-Q4/2019). Patients were categorized into the corresponding mutually exclusive EAC-risk/diagnosis cohorts based on the most advanced stage from GERD to EAC using diagnosis codes in medical claims. Disease-related HRU and costs (2020 USD) were calculated for each cohort. <b>Results:</b> Patients were categorized into the following EAC-risk/diagnosis cohorts: 3 310 385 into GERD, 172 481 into NDBE, 11 516 into IND, 4332 into LGD, 1549 into HGD, and 11 676 into EAC. Disease-related annual mean number of inpatient admissions, office visits, and emergency department visits by cohort were 0.09, 1.45, and 0.19 for GERD; 0.08, 1.55, and 0.10 for NDBE; 0.10, 1.92, and 0.13 for IND; 0.09, 2.05, and 0.10 for LGD; 0.12, 2.16, and 0.14 for HGD; and 1.43, 6.27, and 0.87 for EAC. Disease-related annual mean total healthcare costs by cohort were $6955 for GERD, $8755 for NDBE, $9675 for IND, $12 241 for LGD, $24 239 for HGD, and $146 319 for EAC. <b>Discussion:</b> Patients with GERD, BE, and BERN had important HRU and costs, including inpatient admissions and office visits. As patients progressed to more advanced stages, there was substantially higher disease-related resource utilization, with associated costs being 16 times higher in patients with EAC than those with NDBE. <b>Conclusions:</b> Findings suggest the need for early identification of high-risk individuals prior to progression to EAC to potentially improve clinical and economic outcomes in this population.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"10 1","pages":"51-58"},"PeriodicalIF":2.3000,"publicationDate":"2023-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9985944/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare Resource Utilization and Costs Among Patients With Gastroesophageal Reflux Disease, Barrett's Esophagus, and Barrett's Esophagus-Related Neoplasia in the United States.\",\"authors\":\"Prateek Sharma, Gary W Falk, Menaka Bhor, A Burak Ozbay, Dominick Latremouille-Viau, Annie Guerin, Sherry Shi, Margaret M Elvekrog, Paul Limburg\",\"doi\":\"10.36469/001c.68191\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Gastroesophageal reflux disease (GERD) is a risk factor for Barrett's esophagus (BE) and BE-related neoplasia (BERN). <b>Objectives:</b> This study aimed to evaluate healthcare resource utilization (HRU) and costs associated with GERD, BE, and BERN in the United States. <b>Methods:</b> Adult patients with GERD, nondysplastic BE (NDBE), and BERN (including indefinite for dysplasia [IND], low-grade dysplasia [LGD], high-grade dysplasia [HGD] or esophageal adenocarcinoma [EAC]), were identified from a large US administrative claims database, the IBM Truven Health MarketScan® databases (Q1/2015-Q4/2019). Patients were categorized into the corresponding mutually exclusive EAC-risk/diagnosis cohorts based on the most advanced stage from GERD to EAC using diagnosis codes in medical claims. Disease-related HRU and costs (2020 USD) were calculated for each cohort. <b>Results:</b> Patients were categorized into the following EAC-risk/diagnosis cohorts: 3 310 385 into GERD, 172 481 into NDBE, 11 516 into IND, 4332 into LGD, 1549 into HGD, and 11 676 into EAC. Disease-related annual mean number of inpatient admissions, office visits, and emergency department visits by cohort were 0.09, 1.45, and 0.19 for GERD; 0.08, 1.55, and 0.10 for NDBE; 0.10, 1.92, and 0.13 for IND; 0.09, 2.05, and 0.10 for LGD; 0.12, 2.16, and 0.14 for HGD; and 1.43, 6.27, and 0.87 for EAC. Disease-related annual mean total healthcare costs by cohort were $6955 for GERD, $8755 for NDBE, $9675 for IND, $12 241 for LGD, $24 239 for HGD, and $146 319 for EAC. <b>Discussion:</b> Patients with GERD, BE, and BERN had important HRU and costs, including inpatient admissions and office visits. As patients progressed to more advanced stages, there was substantially higher disease-related resource utilization, with associated costs being 16 times higher in patients with EAC than those with NDBE. <b>Conclusions:</b> Findings suggest the need for early identification of high-risk individuals prior to progression to EAC to potentially improve clinical and economic outcomes in this population.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"10 1\",\"pages\":\"51-58\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-03-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9985944/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36469/001c.68191\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.68191","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Healthcare Resource Utilization and Costs Among Patients With Gastroesophageal Reflux Disease, Barrett's Esophagus, and Barrett's Esophagus-Related Neoplasia in the United States.
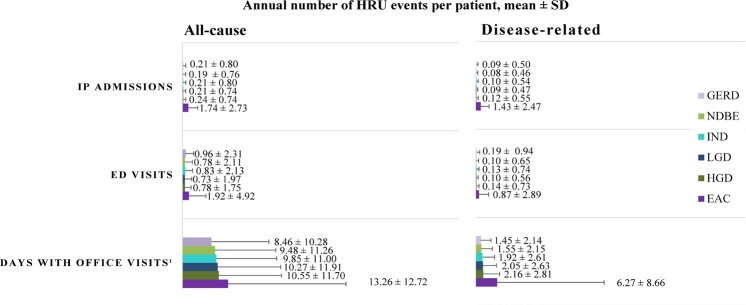
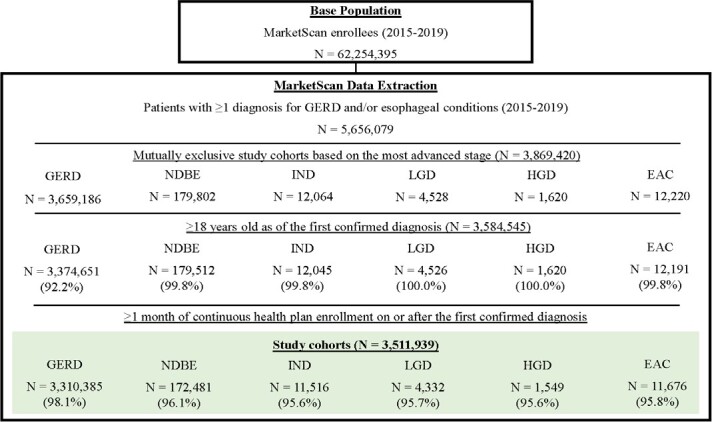
Background: Gastroesophageal reflux disease (GERD) is a risk factor for Barrett's esophagus (BE) and BE-related neoplasia (BERN). Objectives: This study aimed to evaluate healthcare resource utilization (HRU) and costs associated with GERD, BE, and BERN in the United States. Methods: Adult patients with GERD, nondysplastic BE (NDBE), and BERN (including indefinite for dysplasia [IND], low-grade dysplasia [LGD], high-grade dysplasia [HGD] or esophageal adenocarcinoma [EAC]), were identified from a large US administrative claims database, the IBM Truven Health MarketScan® databases (Q1/2015-Q4/2019). Patients were categorized into the corresponding mutually exclusive EAC-risk/diagnosis cohorts based on the most advanced stage from GERD to EAC using diagnosis codes in medical claims. Disease-related HRU and costs (2020 USD) were calculated for each cohort. Results: Patients were categorized into the following EAC-risk/diagnosis cohorts: 3 310 385 into GERD, 172 481 into NDBE, 11 516 into IND, 4332 into LGD, 1549 into HGD, and 11 676 into EAC. Disease-related annual mean number of inpatient admissions, office visits, and emergency department visits by cohort were 0.09, 1.45, and 0.19 for GERD; 0.08, 1.55, and 0.10 for NDBE; 0.10, 1.92, and 0.13 for IND; 0.09, 2.05, and 0.10 for LGD; 0.12, 2.16, and 0.14 for HGD; and 1.43, 6.27, and 0.87 for EAC. Disease-related annual mean total healthcare costs by cohort were $6955 for GERD, $8755 for NDBE, $9675 for IND, $12 241 for LGD, $24 239 for HGD, and $146 319 for EAC. Discussion: Patients with GERD, BE, and BERN had important HRU and costs, including inpatient admissions and office visits. As patients progressed to more advanced stages, there was substantially higher disease-related resource utilization, with associated costs being 16 times higher in patients with EAC than those with NDBE. Conclusions: Findings suggest the need for early identification of high-risk individuals prior to progression to EAC to potentially improve clinical and economic outcomes in this population.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


