Phillip Gu, Eric Clifford, Andrew Gilman, Christopher Chang, Elizabeth Moss, David I Fudman, Phillip Kilgore, Urska Cvek, Marjan Trutschl, J Steven Alexander, Ezra Burstein, Moheb Boktor
{"title":"改善医疗可及性减少贫困IBD患者使用生物治疗的手术需求:“安全网”医院经验。","authors":"Phillip Gu, Eric Clifford, Andrew Gilman, Christopher Chang, Elizabeth Moss, David I Fudman, Phillip Kilgore, Urska Cvek, Marjan Trutschl, J Steven Alexander, Ezra Burstein, Moheb Boktor","doi":"10.3390/pathophysiology29030030","DOIUrl":null,"url":null,"abstract":"<p><p>Low socioeconomic status (SES) is associated with greater morbidity and increased healthcare resource utilization (HRU) in IBD. We examined whether a financial assistance program (FAP) to improve healthcare access affected outcomes and HRU in a cohort of indigent IBD patients requiring biologics. IBD patients (>18 years) receiving care at a ‘safety-net’ hospital who initiated biologics as outpatients between 1 January 2010 and 1 January 2019 were included. Patients were divided by FAP status. Patients without FAP had Medicare, Medicaid, or commercial insurance. Primary outcomes were steroid-free clinical remission at 6 and 12 months. Secondary outcomes were surgery, hospitalization, and ED utilization. Multivariate logistic regression was used to calculate odds ratio (OR) and 95% confidence interval (CI). Decision tree analysis (DTA) was also performed. We included 204 patients with 258 new biologic prescriptions. FAP patients had less complex Crohn’s disease (50.7% vs. 70%, p = 0.033) than non-FAP patients. FAP records indicated fewer prior surgeries (19.6% vs. 38.4% p = 0.003). There were no statistically significant differences in remission rates, disease duration, or days between prescription and receipt of biologics. In multivariable logistic regression, adjusting for baseline demographics and disease severity variables, FAP patients were less likely to undergo surgery (OR: 0.28, 95% CI [0.08−0.91], p = 0.034). DTA suggests that imaging utilization may shed light on surgical differences. We found FAP enrollment was associated with fewer surgeries in a cohort of indigent IBD patients requiring biologics. Further studies are needed to identify interventions to address healthcare disparities in IBD.</p>","PeriodicalId":19852,"journal":{"name":"Pathophysiology","volume":"29 3","pages":"383-393"},"PeriodicalIF":2.7000,"publicationDate":"2022-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9326631/pdf/","citationCount":"2","resultStr":"{\"title\":\"Improved Healthcare Access Reduces Requirements for Surgery in Indigent IBD Patients Using Biologic Therapy: A 'Safety-Net' Hospital Experience.\",\"authors\":\"Phillip Gu, Eric Clifford, Andrew Gilman, Christopher Chang, Elizabeth Moss, David I Fudman, Phillip Kilgore, Urska Cvek, Marjan Trutschl, J Steven Alexander, Ezra Burstein, Moheb Boktor\",\"doi\":\"10.3390/pathophysiology29030030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Low socioeconomic status (SES) is associated with greater morbidity and increased healthcare resource utilization (HRU) in IBD. We examined whether a financial assistance program (FAP) to improve healthcare access affected outcomes and HRU in a cohort of indigent IBD patients requiring biologics. IBD patients (>18 years) receiving care at a ‘safety-net’ hospital who initiated biologics as outpatients between 1 January 2010 and 1 January 2019 were included. Patients were divided by FAP status. Patients without FAP had Medicare, Medicaid, or commercial insurance. Primary outcomes were steroid-free clinical remission at 6 and 12 months. Secondary outcomes were surgery, hospitalization, and ED utilization. Multivariate logistic regression was used to calculate odds ratio (OR) and 95% confidence interval (CI). Decision tree analysis (DTA) was also performed. We included 204 patients with 258 new biologic prescriptions. FAP patients had less complex Crohn’s disease (50.7% vs. 70%, p = 0.033) than non-FAP patients. FAP records indicated fewer prior surgeries (19.6% vs. 38.4% p = 0.003). There were no statistically significant differences in remission rates, disease duration, or days between prescription and receipt of biologics. In multivariable logistic regression, adjusting for baseline demographics and disease severity variables, FAP patients were less likely to undergo surgery (OR: 0.28, 95% CI [0.08−0.91], p = 0.034). DTA suggests that imaging utilization may shed light on surgical differences. We found FAP enrollment was associated with fewer surgeries in a cohort of indigent IBD patients requiring biologics. Further studies are needed to identify interventions to address healthcare disparities in IBD.</p>\",\"PeriodicalId\":19852,\"journal\":{\"name\":\"Pathophysiology\",\"volume\":\"29 3\",\"pages\":\"383-393\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2022-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9326631/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pathophysiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/pathophysiology29030030\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pathophysiology29030030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 2
摘要
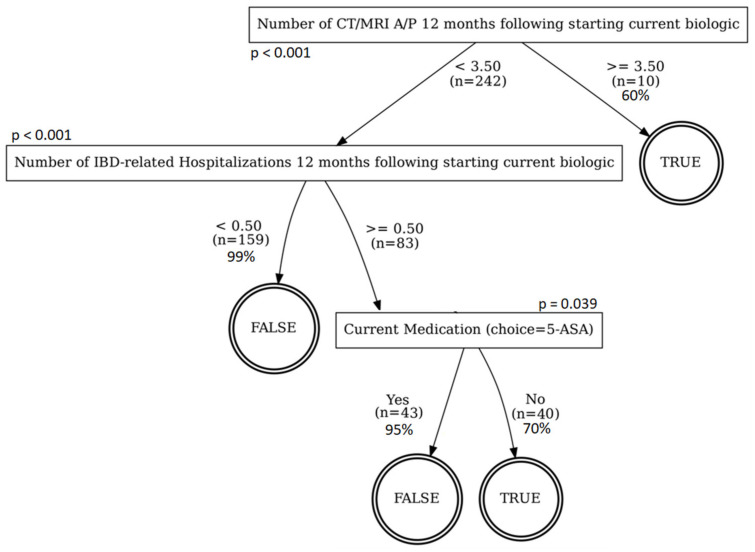
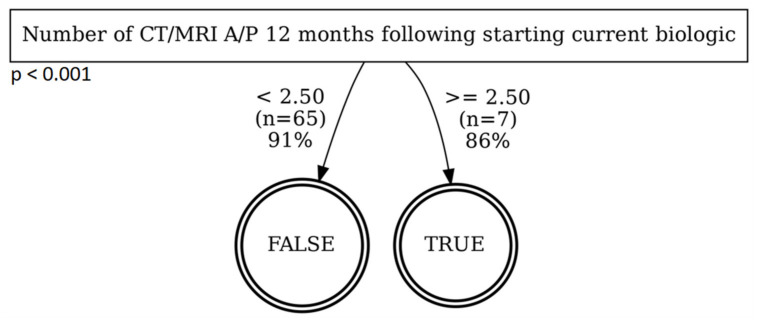
低社会经济地位(SES)与IBD更高的发病率和更高的医疗资源利用率(HRU)相关。我们研究了改善医疗服务可及性的经济援助计划(FAP)是否会影响需要生物制剂的贫困IBD患者队列的结局和HRU。在2010年1月1日至2019年1月1日期间在“安全网”医院接受治疗的IBD患者(>18岁)作为门诊患者开始使用生物制剂。根据FAP状态对患者进行分组。没有FAP的患者有医疗保险、医疗补助或商业保险。主要结果为6个月和12个月无类固醇临床缓解。次要结局是手术、住院和急诊科的使用。采用多因素logistic回归计算优势比(OR)和95%置信区间(CI)。并进行决策树分析(DTA)。我们纳入了204例患者和258个新的生物处方。与非FAP患者相比,FAP患者的复杂克罗恩病较少(50.7% vs 70%, p = 0.033)。FAP记录显示术前手术较少(19.6%比38.4% p = 0.003)。在缓解率、疾病持续时间或服用生物制剂的天数方面,没有统计学上的显著差异。在多变量logistic回归中,调整基线人口统计学和疾病严重程度变量,FAP患者接受手术的可能性较小(OR: 0.28, 95% CI [0.08 - 0.91], p = 0.034)。DTA提示影像学的应用可以揭示手术差异。我们发现,在需要生物制剂的贫困IBD患者队列中,FAP的入组与较少的手术有关。需要进一步的研究来确定干预措施,以解决IBD的医疗保健差异。
Improved Healthcare Access Reduces Requirements for Surgery in Indigent IBD Patients Using Biologic Therapy: A 'Safety-Net' Hospital Experience.
Low socioeconomic status (SES) is associated with greater morbidity and increased healthcare resource utilization (HRU) in IBD. We examined whether a financial assistance program (FAP) to improve healthcare access affected outcomes and HRU in a cohort of indigent IBD patients requiring biologics. IBD patients (>18 years) receiving care at a ‘safety-net’ hospital who initiated biologics as outpatients between 1 January 2010 and 1 January 2019 were included. Patients were divided by FAP status. Patients without FAP had Medicare, Medicaid, or commercial insurance. Primary outcomes were steroid-free clinical remission at 6 and 12 months. Secondary outcomes were surgery, hospitalization, and ED utilization. Multivariate logistic regression was used to calculate odds ratio (OR) and 95% confidence interval (CI). Decision tree analysis (DTA) was also performed. We included 204 patients with 258 new biologic prescriptions. FAP patients had less complex Crohn’s disease (50.7% vs. 70%, p = 0.033) than non-FAP patients. FAP records indicated fewer prior surgeries (19.6% vs. 38.4% p = 0.003). There were no statistically significant differences in remission rates, disease duration, or days between prescription and receipt of biologics. In multivariable logistic regression, adjusting for baseline demographics and disease severity variables, FAP patients were less likely to undergo surgery (OR: 0.28, 95% CI [0.08−0.91], p = 0.034). DTA suggests that imaging utilization may shed light on surgical differences. We found FAP enrollment was associated with fewer surgeries in a cohort of indigent IBD patients requiring biologics. Further studies are needed to identify interventions to address healthcare disparities in IBD.
期刊介绍:
Pathophysiology is an international journal which publishes papers in English which address the etiology, development, and elimination of pathological processes. Contributions on the basic mechanisms underlying these processes, model systems and interdisciplinary approaches are strongly encouraged.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


