Rita Musleh, Peter Schlattmann, Túlio Caldonazo, Hristo Kirov, Otto W Witte, Torsten Doenst, Albrecht Günther, Mahmoud Diab
{"title":"感染性心内膜炎合并颅内出血患者的手术时机:一项系统回顾和荟萃分析。","authors":"Rita Musleh, Peter Schlattmann, Túlio Caldonazo, Hristo Kirov, Otto W Witte, Torsten Doenst, Albrecht Günther, Mahmoud Diab","doi":"10.1161/JAHA.121.024401","DOIUrl":null,"url":null,"abstract":"<p><p>Background Intracranial hemorrhage (ICH) is one of the main causes for lack of surgery in patients with infective endocarditis (IE), despite the presence of surgical indications. We aimed to evaluate the impact of early surgery in patients with IE and with ICH on postoperative neurological deterioration and all-cause mortality and to elucidate the risk of 30-day mortality in patients who were denied surgery. Methods and Results Three libraries (MEDLINE, EMBASE, and Cochrane Library) were assessed. The primary outcome was all-cause mortality, and the secondary outcome was neurological deterioration. Inverse variance method and random model were performed. We identified 16 studies including 355 patients. Nine studies examined the impact of surgical timing (early versus late) and were included in the meta-analysis. Only one study examined the fate of patients with IE and with ICH who were treated conservatively despite having an indication for cardiac surgery, showing higher mortality rates than those who underwent surgery (11.8% versus 2.5%). We found no significant association between early surgery, regardless of its definition, and a higher mortality (odds ratio [OR], 1.69; 95% CI, 0.95-3.02). Early surgery was associated with higher risk for neurological deterioration (OR, 2.00; 95% CI, 1.10-3.65). Conclusions Cardiac surgery for IE within 30 days of ICH was not associated with higher mortality, but with an increased rate of neurological deterioration. The 30-day mortality in patients with IE and with ICH who were denied surgery has not yet been sufficiently investigated. This patient group should be analyzed in future studies in more detail.</p>","PeriodicalId":17189,"journal":{"name":"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease","volume":"17 1","pages":"e024401"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9238556/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Timing in Patients With Infective Endocarditis and With Intracranial Hemorrhage: A Systematic Review and Meta-Analysis.\",\"authors\":\"Rita Musleh, Peter Schlattmann, Túlio Caldonazo, Hristo Kirov, Otto W Witte, Torsten Doenst, Albrecht Günther, Mahmoud Diab\",\"doi\":\"10.1161/JAHA.121.024401\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Background Intracranial hemorrhage (ICH) is one of the main causes for lack of surgery in patients with infective endocarditis (IE), despite the presence of surgical indications. We aimed to evaluate the impact of early surgery in patients with IE and with ICH on postoperative neurological deterioration and all-cause mortality and to elucidate the risk of 30-day mortality in patients who were denied surgery. Methods and Results Three libraries (MEDLINE, EMBASE, and Cochrane Library) were assessed. The primary outcome was all-cause mortality, and the secondary outcome was neurological deterioration. Inverse variance method and random model were performed. We identified 16 studies including 355 patients. Nine studies examined the impact of surgical timing (early versus late) and were included in the meta-analysis. Only one study examined the fate of patients with IE and with ICH who were treated conservatively despite having an indication for cardiac surgery, showing higher mortality rates than those who underwent surgery (11.8% versus 2.5%). We found no significant association between early surgery, regardless of its definition, and a higher mortality (odds ratio [OR], 1.69; 95% CI, 0.95-3.02). Early surgery was associated with higher risk for neurological deterioration (OR, 2.00; 95% CI, 1.10-3.65). Conclusions Cardiac surgery for IE within 30 days of ICH was not associated with higher mortality, but with an increased rate of neurological deterioration. The 30-day mortality in patients with IE and with ICH who were denied surgery has not yet been sufficiently investigated. This patient group should be analyzed in future studies in more detail.</p>\",\"PeriodicalId\":17189,\"journal\":{\"name\":\"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease\",\"volume\":\"17 1\",\"pages\":\"e024401\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9238556/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1161/JAHA.121.024401\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/5/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1161/JAHA.121.024401","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Surgical Timing in Patients With Infective Endocarditis and With Intracranial Hemorrhage: A Systematic Review and Meta-Analysis.
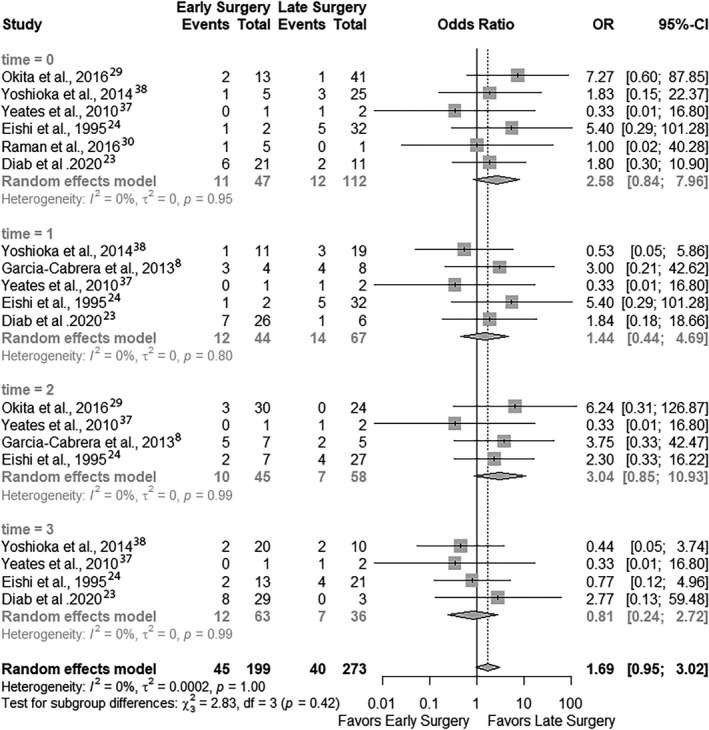
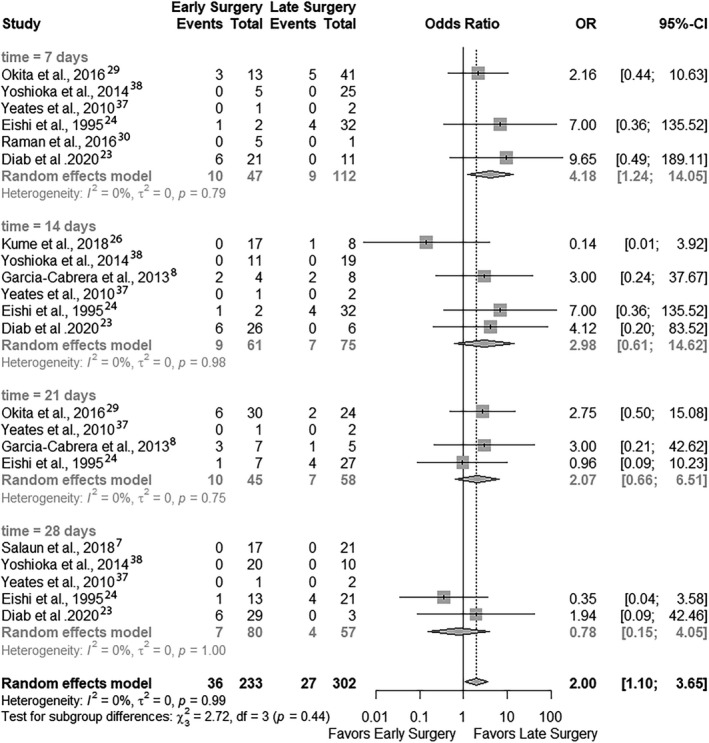
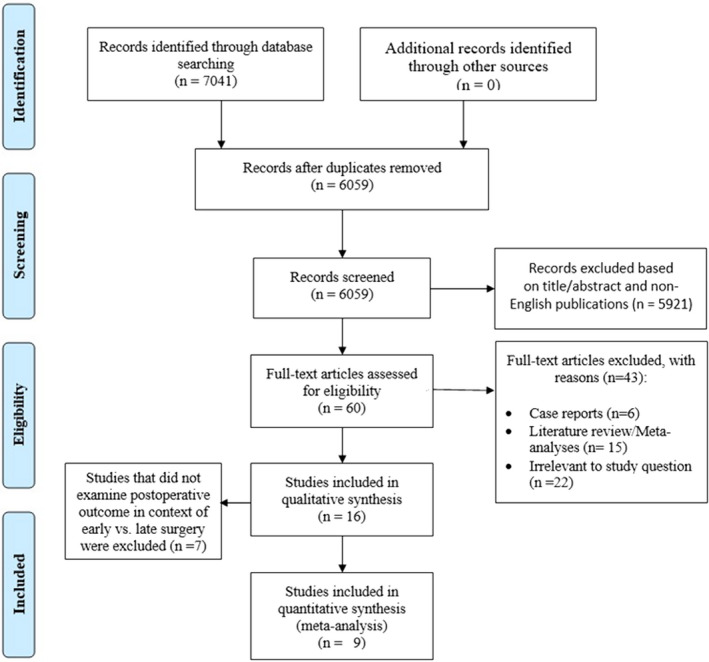
Background Intracranial hemorrhage (ICH) is one of the main causes for lack of surgery in patients with infective endocarditis (IE), despite the presence of surgical indications. We aimed to evaluate the impact of early surgery in patients with IE and with ICH on postoperative neurological deterioration and all-cause mortality and to elucidate the risk of 30-day mortality in patients who were denied surgery. Methods and Results Three libraries (MEDLINE, EMBASE, and Cochrane Library) were assessed. The primary outcome was all-cause mortality, and the secondary outcome was neurological deterioration. Inverse variance method and random model were performed. We identified 16 studies including 355 patients. Nine studies examined the impact of surgical timing (early versus late) and were included in the meta-analysis. Only one study examined the fate of patients with IE and with ICH who were treated conservatively despite having an indication for cardiac surgery, showing higher mortality rates than those who underwent surgery (11.8% versus 2.5%). We found no significant association between early surgery, regardless of its definition, and a higher mortality (odds ratio [OR], 1.69; 95% CI, 0.95-3.02). Early surgery was associated with higher risk for neurological deterioration (OR, 2.00; 95% CI, 1.10-3.65). Conclusions Cardiac surgery for IE within 30 days of ICH was not associated with higher mortality, but with an increased rate of neurological deterioration. The 30-day mortality in patients with IE and with ICH who were denied surgery has not yet been sufficiently investigated. This patient group should be analyzed in future studies in more detail.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


