Jaume Figueras, Jordi Bañeras, Carlos Peña-Gil, José A Barrabés, Jose Rodriguez Palomares, David Garcia Dorado
{"title":"有冠状动脉疾病和无冠状动脉疾病的急性肺水肿患者的住院和 4 年死亡率预测因素。","authors":"Jaume Figueras, Jordi Bañeras, Carlos Peña-Gil, José A Barrabés, Jose Rodriguez Palomares, David Garcia Dorado","doi":"10.1161/JAHA.115.002581","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Long-term prognosis of acute pulmonary edema (APE) remains ill defined.</p><p><strong>Methods and results: </strong>We evaluated demographic, echocardiographic, and angiographic data of 806 consecutive patients with APE with (CAD) and without coronary artery disease (non-CAD) admitted from 2000 to 2010. Differences between hospital and long-term mortality and its predictors were also assessed. CAD patients (n=638) were older and had higher incidence of diabetes and peripheral vascular disease than non-CAD (n=168), and lower ejection fraction. Hospital mortality was similar in both groups (26.5% vs 31.5%; P=0.169) but APE recurrence was higher in CAD patients (17.3% vs 6.5%; P<0.001). Age, admission systolic blood pressure, recurrence of APE, and need for inotropics or endotracheal intubation were the main independent predictors of hospital mortality. In contrast, overall mortality (70.0% vs 57.1%; P=0.002) and readmission for nonfatal heart failure after a 45-month follow-up (10-140; 17.3% vs 7.6%; P=0.009) were higher in CAD than in non-CAD patients. Age, peripheral vascular disease, and peak creatine kinase MB during index hospitalization, but not ejection fraction, were the main independent predictors of overall mortality, whereas coronary revascularization or valvular surgery were protective. These interventions were mostly performed during hospitalization index (294 of 307; 96%) and not intervened patients showed a higher risk profile.</p><p><strong>Conclusions: </strong>Long-term mortality in APE is high and higher in CAD than in non-CAD patients. Considering the different in-hospital and long-term mortality predictors herein described, which do not necessarily involve systolic function, it is conceivable that a more aggressive interventional program might improve survival in high-risk patients.</p>","PeriodicalId":70695,"journal":{"name":"现代水文学期刊(英文)","volume":"7 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2016-02-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4802455/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hospital and 4-Year Mortality Predictors in Patients With Acute Pulmonary Edema With and Without Coronary Artery Disease.\",\"authors\":\"Jaume Figueras, Jordi Bañeras, Carlos Peña-Gil, José A Barrabés, Jose Rodriguez Palomares, David Garcia Dorado\",\"doi\":\"10.1161/JAHA.115.002581\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Long-term prognosis of acute pulmonary edema (APE) remains ill defined.</p><p><strong>Methods and results: </strong>We evaluated demographic, echocardiographic, and angiographic data of 806 consecutive patients with APE with (CAD) and without coronary artery disease (non-CAD) admitted from 2000 to 2010. Differences between hospital and long-term mortality and its predictors were also assessed. CAD patients (n=638) were older and had higher incidence of diabetes and peripheral vascular disease than non-CAD (n=168), and lower ejection fraction. Hospital mortality was similar in both groups (26.5% vs 31.5%; P=0.169) but APE recurrence was higher in CAD patients (17.3% vs 6.5%; P<0.001). Age, admission systolic blood pressure, recurrence of APE, and need for inotropics or endotracheal intubation were the main independent predictors of hospital mortality. In contrast, overall mortality (70.0% vs 57.1%; P=0.002) and readmission for nonfatal heart failure after a 45-month follow-up (10-140; 17.3% vs 7.6%; P=0.009) were higher in CAD than in non-CAD patients. Age, peripheral vascular disease, and peak creatine kinase MB during index hospitalization, but not ejection fraction, were the main independent predictors of overall mortality, whereas coronary revascularization or valvular surgery were protective. These interventions were mostly performed during hospitalization index (294 of 307; 96%) and not intervened patients showed a higher risk profile.</p><p><strong>Conclusions: </strong>Long-term mortality in APE is high and higher in CAD than in non-CAD patients. Considering the different in-hospital and long-term mortality predictors herein described, which do not necessarily involve systolic function, it is conceivable that a more aggressive interventional program might improve survival in high-risk patients.</p>\",\"PeriodicalId\":70695,\"journal\":{\"name\":\"现代水文学期刊(英文)\",\"volume\":\"7 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-02-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4802455/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"现代水文学期刊(英文)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1161/JAHA.115.002581\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"现代水文学期刊(英文)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1161/JAHA.115.002581","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
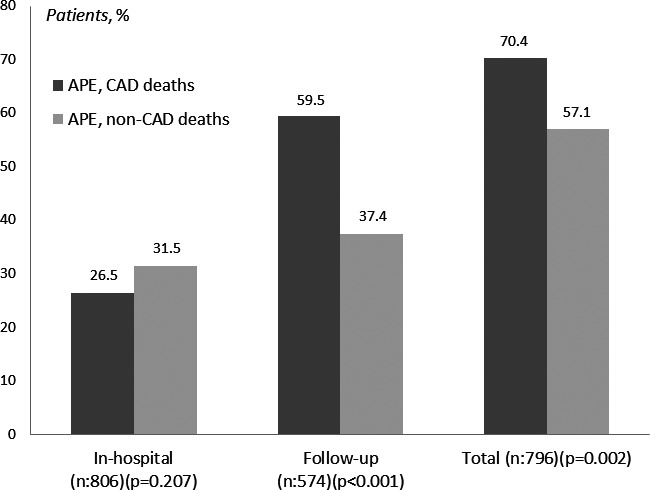
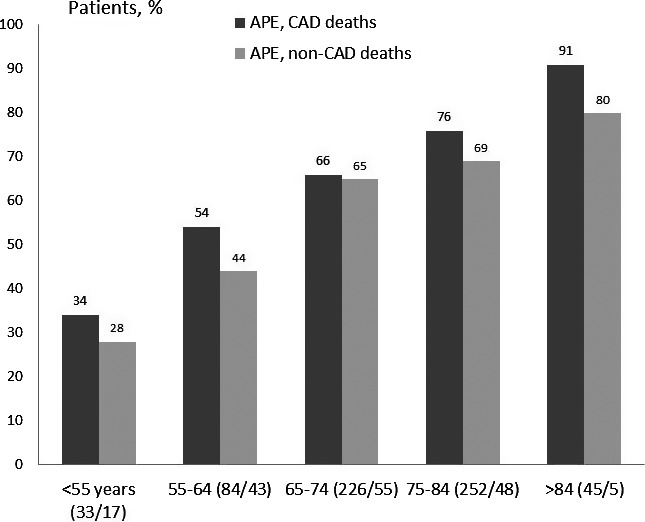
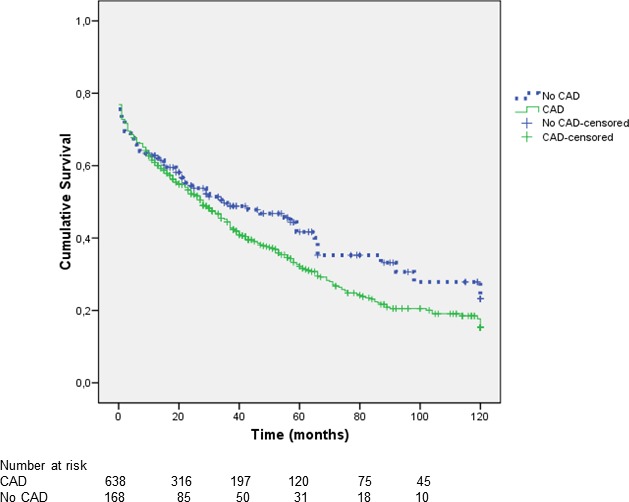
Methods and results: We evaluated demographic, echocardiographic, and angiographic data of 806 consecutive patients with APE with (CAD) and without coronary artery disease (non-CAD) admitted from 2000 to 2010. Differences between hospital and long-term mortality and its predictors were also assessed. CAD patients (n=638) were older and had higher incidence of diabetes and peripheral vascular disease than non-CAD (n=168), and lower ejection fraction. Hospital mortality was similar in both groups (26.5% vs 31.5%; P=0.169) but APE recurrence was higher in CAD patients (17.3% vs 6.5%; P<0.001). Age, admission systolic blood pressure, recurrence of APE, and need for inotropics or endotracheal intubation were the main independent predictors of hospital mortality. In contrast, overall mortality (70.0% vs 57.1%; P=0.002) and readmission for nonfatal heart failure after a 45-month follow-up (10-140; 17.3% vs 7.6%; P=0.009) were higher in CAD than in non-CAD patients. Age, peripheral vascular disease, and peak creatine kinase MB during index hospitalization, but not ejection fraction, were the main independent predictors of overall mortality, whereas coronary revascularization or valvular surgery were protective. These interventions were mostly performed during hospitalization index (294 of 307; 96%) and not intervened patients showed a higher risk profile.
Conclusions: Long-term mortality in APE is high and higher in CAD than in non-CAD patients. Considering the different in-hospital and long-term mortality predictors herein described, which do not necessarily involve systolic function, it is conceivable that a more aggressive interventional program might improve survival in high-risk patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


