Karin Cerna, Dana Duricova, Martin Lukas, Martin Kolar, Nadezda Machkova, Veronika Hruba, Katarina Mitrova, Kristyna Kubickova, Marta Kostrejova, Jakub Jirsa, Kristyna Kastylova, Stepan Peterka, Gabriela Vojtechova, Milan Lukas
{"title":"皮下英夫利昔单抗治疗难治性克罗恩病患者:一种可能的生物better?","authors":"Karin Cerna, Dana Duricova, Martin Lukas, Martin Kolar, Nadezda Machkova, Veronika Hruba, Katarina Mitrova, Kristyna Kubickova, Marta Kostrejova, Jakub Jirsa, Kristyna Kastylova, Stepan Peterka, Gabriela Vojtechova, Milan Lukas","doi":"10.1093/crocol/otad040","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A subcutaneous formulation of infliximab (IFX-SC) approved to treat patients with inflammatory bowel disease may offer improved efficacy versus intravenous infliximab.</p><p><strong>Methods: </strong>Patients with refractory Crohn's disease (CD, <i>n</i> = 32) previously treated unsuccessfully with at least 2 biologics were treated with IFX-SC and followed from baseline at Week 0 (W0) to Week 30 (W30). The study's primary endpoint was the treatment's persistence at W30, while secondary goals included the analysis of serum infliximab trough levels (TL IFX), dynamics of anti-IFX antibodies (ATIs), and clinical, serum and fecal markers of CD activity during IFX-SC treatment.</p><p><strong>Results: </strong>Midterm treatment persistence with the continuation of treatment after W30 was 53%. TL IFX median values showed rapid, significant upward dynamics and exceeded 15.5 μg/mL at W30, whereas median ATI levels significantly declined. Among ATI-negative patients at W0 (<i>n</i> = 15), only one showed IFX immunogenicity with newly developed ATIs at W30. Among ATI-positive patients at W0, ATI seroconversion from ATI-positive to ATI-negative status was observed in 10 of 17 patients (58.8%). Patients who had continued IFX-SC treatment at W30 showed significant decreases in C-reactive protein (<i>P</i> = .0341), fecal calprotectin (<i>P</i> = .0002), and Harvey-Bradshaw index (<i>P =</i> .0029) since W0.</p><p><strong>Conclusions: </strong>Patients with refractory CD previously treated with at least 2 biologics exhibited clinically relevant improvement with IFX-SC, which showed less immunogenic potential than IFX-IV and highly stable TL IFX.</p>","PeriodicalId":37025,"journal":{"name":"Geoenvironmental Disasters","volume":"4 1","pages":"otad040"},"PeriodicalIF":4.0000,"publicationDate":"2023-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10640858/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subcutaneous Infliximab in Refractory Crohn's Disease Patients: A Possible Biobetter?\",\"authors\":\"Karin Cerna, Dana Duricova, Martin Lukas, Martin Kolar, Nadezda Machkova, Veronika Hruba, Katarina Mitrova, Kristyna Kubickova, Marta Kostrejova, Jakub Jirsa, Kristyna Kastylova, Stepan Peterka, Gabriela Vojtechova, Milan Lukas\",\"doi\":\"10.1093/crocol/otad040\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A subcutaneous formulation of infliximab (IFX-SC) approved to treat patients with inflammatory bowel disease may offer improved efficacy versus intravenous infliximab.</p><p><strong>Methods: </strong>Patients with refractory Crohn's disease (CD, <i>n</i> = 32) previously treated unsuccessfully with at least 2 biologics were treated with IFX-SC and followed from baseline at Week 0 (W0) to Week 30 (W30). The study's primary endpoint was the treatment's persistence at W30, while secondary goals included the analysis of serum infliximab trough levels (TL IFX), dynamics of anti-IFX antibodies (ATIs), and clinical, serum and fecal markers of CD activity during IFX-SC treatment.</p><p><strong>Results: </strong>Midterm treatment persistence with the continuation of treatment after W30 was 53%. TL IFX median values showed rapid, significant upward dynamics and exceeded 15.5 μg/mL at W30, whereas median ATI levels significantly declined. Among ATI-negative patients at W0 (<i>n</i> = 15), only one showed IFX immunogenicity with newly developed ATIs at W30. Among ATI-positive patients at W0, ATI seroconversion from ATI-positive to ATI-negative status was observed in 10 of 17 patients (58.8%). Patients who had continued IFX-SC treatment at W30 showed significant decreases in C-reactive protein (<i>P</i> = .0341), fecal calprotectin (<i>P</i> = .0002), and Harvey-Bradshaw index (<i>P =</i> .0029) since W0.</p><p><strong>Conclusions: </strong>Patients with refractory CD previously treated with at least 2 biologics exhibited clinically relevant improvement with IFX-SC, which showed less immunogenic potential than IFX-IV and highly stable TL IFX.</p>\",\"PeriodicalId\":37025,\"journal\":{\"name\":\"Geoenvironmental Disasters\",\"volume\":\"4 1\",\"pages\":\"otad040\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10640858/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Geoenvironmental Disasters\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otad040\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENVIRONMENTAL SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geoenvironmental Disasters","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad040","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENVIRONMENTAL SCIENCES","Score":null,"Total":0}
Subcutaneous Infliximab in Refractory Crohn's Disease Patients: A Possible Biobetter?
Background: A subcutaneous formulation of infliximab (IFX-SC) approved to treat patients with inflammatory bowel disease may offer improved efficacy versus intravenous infliximab.
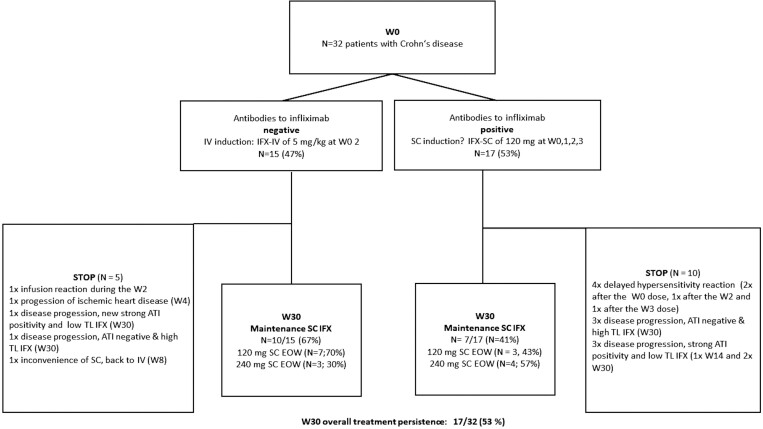
Methods: Patients with refractory Crohn's disease (CD, n = 32) previously treated unsuccessfully with at least 2 biologics were treated with IFX-SC and followed from baseline at Week 0 (W0) to Week 30 (W30). The study's primary endpoint was the treatment's persistence at W30, while secondary goals included the analysis of serum infliximab trough levels (TL IFX), dynamics of anti-IFX antibodies (ATIs), and clinical, serum and fecal markers of CD activity during IFX-SC treatment.
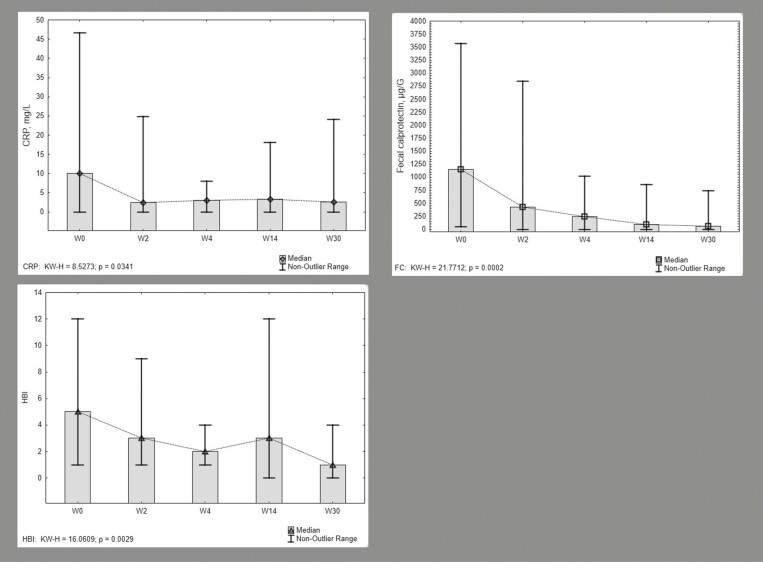
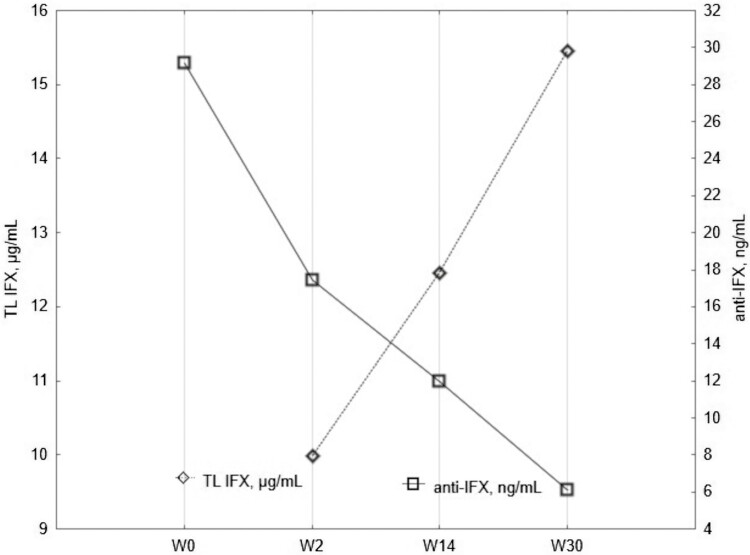
Results: Midterm treatment persistence with the continuation of treatment after W30 was 53%. TL IFX median values showed rapid, significant upward dynamics and exceeded 15.5 μg/mL at W30, whereas median ATI levels significantly declined. Among ATI-negative patients at W0 (n = 15), only one showed IFX immunogenicity with newly developed ATIs at W30. Among ATI-positive patients at W0, ATI seroconversion from ATI-positive to ATI-negative status was observed in 10 of 17 patients (58.8%). Patients who had continued IFX-SC treatment at W30 showed significant decreases in C-reactive protein (P = .0341), fecal calprotectin (P = .0002), and Harvey-Bradshaw index (P = .0029) since W0.
Conclusions: Patients with refractory CD previously treated with at least 2 biologics exhibited clinically relevant improvement with IFX-SC, which showed less immunogenic potential than IFX-IV and highly stable TL IFX.
期刊介绍:
Geoenvironmental Disasters is an international journal with a focus on multi-disciplinary applied and fundamental research and the effects and impacts on infrastructure, society and the environment of geoenvironmental disasters triggered by various types of geo-hazards (e.g. earthquakes, volcanic activity, landslides, tsunamis, intensive erosion and hydro-meteorological events).
The integrated study of Geoenvironmental Disasters is an emerging and composite field of research interfacing with areas traditionally within civil engineering, earth sciences, atmospheric sciences and the life sciences. It centers on the interactions within and between the Earth''s ground, air and water environments, all of which are affected by climate, geological, morphological and anthropological processes; and biological and ecological cycles. Disasters are dynamic forces which can change the Earth pervasively, rapidly, or abruptly, and which can generate lasting effects on the natural and built environments.
The journal publishes research papers, case studies and quick reports of recent geoenvironmental disasters, review papers and technical reports of various geoenvironmental disaster-related case studies. The focus on case studies and quick reports of recent geoenvironmental disasters helps to advance the practical understanding of geoenvironmental disasters and to inform future research priorities; they are a major component of the journal. The journal aims for the rapid publication of research papers at a high scientific level. The journal welcomes proposals for special issues reflecting the trends in geoenvironmental disaster reduction and monothematic issues. Researchers and practitioners are encouraged to submit original, unpublished contributions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


