{"title":"阴道内宫内睾丸扭转1例。","authors":"Murad Habib, Muhammad Bin Amjad, Mansoor Ahmed","doi":"10.1515/crpm-2022-0013","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Intrauterine testicular torsion is extremely rare and the exact cause remains largely unknown. It is the result of an ischemic insult intrauterine, which presents as either extra-vaginal or intravaginal testicular torsion. Urgent surgical exploration and fixating the contralateral testis is key in the management of this condition.</p><p><strong>Case presentation: </strong>We present here the case of a two-day old neonate with in-born right scrotal swelling admitted at Children's hospital. The patient was born at term via cesarean section at a private hospital. Upon arrival in the emergency department, he was well hydrated, pink at room temperature with good perfusion. Upon examination, the right testis was found to be enlarged, tense, non-tender visibly reddish with overlying skin excoriation. Trans-illumination was negative in right but positive in the contralateral testis. Both hernial orifices were normal. Doppler ultrasound of the inguinoscrotal area found the right testis to be enlarged (15.6*9.4 mm) and showed heterogeneous hypoechoic texture with prominent rete testis and no flow on color doppler analysis. An urgent scrotal exploration was undertaken. Intra-operatively there was frank necrotic right testis with intravaginal torsion of the testis and minimal hydrocele. A right orchidectomy and contralateral orchidopexy were performed.</p><p><strong>Conclusions: </strong>Intrauterine testicular torsion should be treated as a surgical emergency. We advocate early recognition of intrauterine testicular torsion, alongside surgical exploration and simultaneous contralateral orchidopexy.</p>","PeriodicalId":9617,"journal":{"name":"Case Reports in Perinatal Medicine","volume":"73 1","pages":"20220013"},"PeriodicalIF":0.2000,"publicationDate":"2022-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11616535/pdf/","citationCount":"0","resultStr":"{\"title\":\"A case of intra-vaginal intrauterine testicular torsion.\",\"authors\":\"Murad Habib, Muhammad Bin Amjad, Mansoor Ahmed\",\"doi\":\"10.1515/crpm-2022-0013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Intrauterine testicular torsion is extremely rare and the exact cause remains largely unknown. It is the result of an ischemic insult intrauterine, which presents as either extra-vaginal or intravaginal testicular torsion. Urgent surgical exploration and fixating the contralateral testis is key in the management of this condition.</p><p><strong>Case presentation: </strong>We present here the case of a two-day old neonate with in-born right scrotal swelling admitted at Children's hospital. The patient was born at term via cesarean section at a private hospital. Upon arrival in the emergency department, he was well hydrated, pink at room temperature with good perfusion. Upon examination, the right testis was found to be enlarged, tense, non-tender visibly reddish with overlying skin excoriation. Trans-illumination was negative in right but positive in the contralateral testis. Both hernial orifices were normal. Doppler ultrasound of the inguinoscrotal area found the right testis to be enlarged (15.6*9.4 mm) and showed heterogeneous hypoechoic texture with prominent rete testis and no flow on color doppler analysis. An urgent scrotal exploration was undertaken. Intra-operatively there was frank necrotic right testis with intravaginal torsion of the testis and minimal hydrocele. A right orchidectomy and contralateral orchidopexy were performed.</p><p><strong>Conclusions: </strong>Intrauterine testicular torsion should be treated as a surgical emergency. We advocate early recognition of intrauterine testicular torsion, alongside surgical exploration and simultaneous contralateral orchidopexy.</p>\",\"PeriodicalId\":9617,\"journal\":{\"name\":\"Case Reports in Perinatal Medicine\",\"volume\":\"73 1\",\"pages\":\"20220013\"},\"PeriodicalIF\":0.2000,\"publicationDate\":\"2022-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11616535/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Perinatal Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/crpm-2022-0013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Perinatal Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/crpm-2022-0013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
A case of intra-vaginal intrauterine testicular torsion.
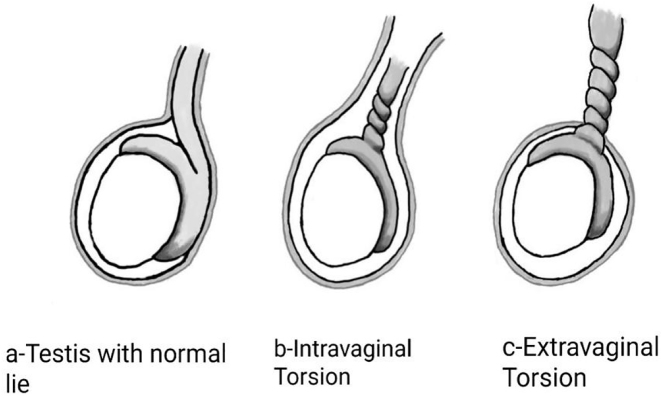
Objectives: Intrauterine testicular torsion is extremely rare and the exact cause remains largely unknown. It is the result of an ischemic insult intrauterine, which presents as either extra-vaginal or intravaginal testicular torsion. Urgent surgical exploration and fixating the contralateral testis is key in the management of this condition.
Case presentation: We present here the case of a two-day old neonate with in-born right scrotal swelling admitted at Children's hospital. The patient was born at term via cesarean section at a private hospital. Upon arrival in the emergency department, he was well hydrated, pink at room temperature with good perfusion. Upon examination, the right testis was found to be enlarged, tense, non-tender visibly reddish with overlying skin excoriation. Trans-illumination was negative in right but positive in the contralateral testis. Both hernial orifices were normal. Doppler ultrasound of the inguinoscrotal area found the right testis to be enlarged (15.6*9.4 mm) and showed heterogeneous hypoechoic texture with prominent rete testis and no flow on color doppler analysis. An urgent scrotal exploration was undertaken. Intra-operatively there was frank necrotic right testis with intravaginal torsion of the testis and minimal hydrocele. A right orchidectomy and contralateral orchidopexy were performed.
Conclusions: Intrauterine testicular torsion should be treated as a surgical emergency. We advocate early recognition of intrauterine testicular torsion, alongside surgical exploration and simultaneous contralateral orchidopexy.
期刊介绍:
Case Reports in Perinatal Medicine is a double-blind peer-reviewed journal. The objective of the new journal is very similar to that of JPM. In addition to evidence-based studies, practitioners in clinical practice esteem especially exemplary reports of cases that reveal specific manifestations of diseases, its progress or its treatment. We consider case reports and series to be brief reports describing an isolated clinical case or a small number of cases. They may describe new or uncommon diagnoses, unusual outcomes or prognosis, new or infrequently used therapies and side effects of therapy not usually discovered in clinical trials. They represent the basic concept of experiences for studies on representative groups for further evidence-based research. The potential roles of case reports and case series are: Recognition and description of new diseases Detection of drug side effects (adverse or beneficial) Study of mechanisms of disease Medical education and audit Recognition of rare manifestations of disease.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


