Oliver van Hecke, Alice Fuller, Clare Bankhead, Sara Jenkins-Jones, Nick Francis, Michael Moore, Chris Butler, Kay Wang
{"title":"抗生素暴露和随后呼吸道感染的“反应失败”:一项对英国初级保健学龄前儿童的观察性队列研究。","authors":"Oliver van Hecke, Alice Fuller, Clare Bankhead, Sara Jenkins-Jones, Nick Francis, Michael Moore, Chris Butler, Kay Wang","doi":"10.3399/bjgp19X705089","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Childhood antibiotic exposure has important clinically relevant implications. These include disruption to the microbiome, antibiotic resistance, and clinical workload manifesting as treatment 'failure'.</p><p><strong>Aim: </strong>To examine the relationship between the number of antibiotic courses prescribed to preschool children for acute respiratory tract infections (RTI), in the preceding year, and subsequent RTIs that failed to respond to antibiotic treatment ('response failures').</p><p><strong>Design and setting: </strong>A cohort study using UK primary care data from the Clinical Practice Research Datalink, 2009 to 2016.</p><p><strong>Method: </strong>Children aged 12 to 60 months (1 to 5 years) who were prescribed an antibiotic for an acute RTI (upper and lower RTI or otitis media) were included. One random index antibiotic course for RTI per child was selected. Exposure was the number of antibiotic prescriptions for acute RTI up to 12 months before the index antibiotic prescription. The outcome was 'response failure' up to 14 days after index antibiotic prescription, defined as: subsequent antibiotic prescription; referral; hospital admission; death; or emergency department attendance within 3 days. The authors used logistic regression models to estimate the odds between antibiotic exposure and response failure.</p><p><strong>Results: </strong>Out of 114 329 children who were prescribed an antibiotic course for acute RTI, children who received ≥2 antibiotic courses for acute RTIs in the preceding year had greater odds of response failure; one antibiotic course: adjusted odds ratio (OR) 1.03 (95% confidence interval [CI] = 0.88 to 1.21), <i>P</i> = 0.67, <i>n</i> = 230 children; ≥2 antibiotic courses: adjusted OR 1.32 (CI = 1.04 to 1.66), <i>P</i> = 0.02, <i>n</i> = 97.</p><p><strong>Conclusion: </strong>Childhood antibiotic exposure for acute RTI may be a good predictor for subsequent response failure (but not necessarily because of antibiotic treatment failure). Further research is needed to improve understanding of the mechanisms underlying response failure.</p>","PeriodicalId":22333,"journal":{"name":"The British Journal of General Practice","volume":"45 1","pages":"e638-e646"},"PeriodicalIF":0.0000,"publicationDate":"2019-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6692084/pdf/","citationCount":"0","resultStr":"{\"title\":\"Antibiotic exposure and 'response failure' for subsequent respiratory tract infections: an observational cohort study of UK preschool children in primary care.\",\"authors\":\"Oliver van Hecke, Alice Fuller, Clare Bankhead, Sara Jenkins-Jones, Nick Francis, Michael Moore, Chris Butler, Kay Wang\",\"doi\":\"10.3399/bjgp19X705089\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Childhood antibiotic exposure has important clinically relevant implications. These include disruption to the microbiome, antibiotic resistance, and clinical workload manifesting as treatment 'failure'.</p><p><strong>Aim: </strong>To examine the relationship between the number of antibiotic courses prescribed to preschool children for acute respiratory tract infections (RTI), in the preceding year, and subsequent RTIs that failed to respond to antibiotic treatment ('response failures').</p><p><strong>Design and setting: </strong>A cohort study using UK primary care data from the Clinical Practice Research Datalink, 2009 to 2016.</p><p><strong>Method: </strong>Children aged 12 to 60 months (1 to 5 years) who were prescribed an antibiotic for an acute RTI (upper and lower RTI or otitis media) were included. One random index antibiotic course for RTI per child was selected. Exposure was the number of antibiotic prescriptions for acute RTI up to 12 months before the index antibiotic prescription. The outcome was 'response failure' up to 14 days after index antibiotic prescription, defined as: subsequent antibiotic prescription; referral; hospital admission; death; or emergency department attendance within 3 days. The authors used logistic regression models to estimate the odds between antibiotic exposure and response failure.</p><p><strong>Results: </strong>Out of 114 329 children who were prescribed an antibiotic course for acute RTI, children who received ≥2 antibiotic courses for acute RTIs in the preceding year had greater odds of response failure; one antibiotic course: adjusted odds ratio (OR) 1.03 (95% confidence interval [CI] = 0.88 to 1.21), <i>P</i> = 0.67, <i>n</i> = 230 children; ≥2 antibiotic courses: adjusted OR 1.32 (CI = 1.04 to 1.66), <i>P</i> = 0.02, <i>n</i> = 97.</p><p><strong>Conclusion: </strong>Childhood antibiotic exposure for acute RTI may be a good predictor for subsequent response failure (but not necessarily because of antibiotic treatment failure). Further research is needed to improve understanding of the mechanisms underlying response failure.</p>\",\"PeriodicalId\":22333,\"journal\":{\"name\":\"The British Journal of General Practice\",\"volume\":\"45 1\",\"pages\":\"e638-e646\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6692084/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The British Journal of General Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3399/bjgp19X705089\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/9/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The British Journal of General Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3399/bjgp19X705089","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/9/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:儿童抗生素暴露具有重要的临床意义。这些包括微生物群的破坏、抗生素耐药性和临床工作量表现为治疗“失败”。目的:研究前一年学龄前儿童急性呼吸道感染(RTI)的抗生素疗程数与随后对抗生素治疗无效的RTIs(“反应失败”)之间的关系。设计和背景:一项队列研究,使用2009年至2016年临床实践研究数据链中的英国初级保健数据。方法:年龄在12至60个月(1至5岁)的儿童,因急性呼吸道感染(上、下呼吸道感染或中耳炎)服用抗生素。每个儿童随机选择一个RTI指标抗生素疗程。暴露量是指在指数抗生素处方前12个月的急性呼吸道感染抗生素处方数量。结果为指标抗生素处方后14天“反应失败”,定义为:后续抗生素处方;推荐;住院;死亡;或3天内到急诊科就诊。作者使用逻辑回归模型来估计抗生素暴露和反应失败之间的几率。结果:在114329名因急性呼吸道感染而接受抗生素治疗的儿童中,前一年接受≥2个抗生素治疗的儿童反应失败的几率更大;一个抗生素疗程:调整优势比(OR) 1.03(95%可信区间[CI] = 0.88 ~ 1.21), P = 0.67, n = 230名儿童;≥2个抗生素疗程:调整OR为1.32 (CI = 1.04 ~ 1.66), P = 0.02, n = 97。结论:急性呼吸道感染的儿童抗生素暴露可能是随后反应失败的良好预测因素(但不一定是因为抗生素治疗失败)。需要进一步的研究来提高对反应失败机制的理解。
Antibiotic exposure and 'response failure' for subsequent respiratory tract infections: an observational cohort study of UK preschool children in primary care.
Background: Childhood antibiotic exposure has important clinically relevant implications. These include disruption to the microbiome, antibiotic resistance, and clinical workload manifesting as treatment 'failure'.
Aim: To examine the relationship between the number of antibiotic courses prescribed to preschool children for acute respiratory tract infections (RTI), in the preceding year, and subsequent RTIs that failed to respond to antibiotic treatment ('response failures').
Design and setting: A cohort study using UK primary care data from the Clinical Practice Research Datalink, 2009 to 2016.
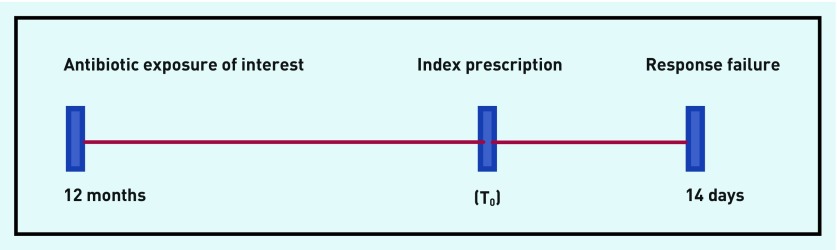
Method: Children aged 12 to 60 months (1 to 5 years) who were prescribed an antibiotic for an acute RTI (upper and lower RTI or otitis media) were included. One random index antibiotic course for RTI per child was selected. Exposure was the number of antibiotic prescriptions for acute RTI up to 12 months before the index antibiotic prescription. The outcome was 'response failure' up to 14 days after index antibiotic prescription, defined as: subsequent antibiotic prescription; referral; hospital admission; death; or emergency department attendance within 3 days. The authors used logistic regression models to estimate the odds between antibiotic exposure and response failure.
Results: Out of 114 329 children who were prescribed an antibiotic course for acute RTI, children who received ≥2 antibiotic courses for acute RTIs in the preceding year had greater odds of response failure; one antibiotic course: adjusted odds ratio (OR) 1.03 (95% confidence interval [CI] = 0.88 to 1.21), P = 0.67, n = 230 children; ≥2 antibiotic courses: adjusted OR 1.32 (CI = 1.04 to 1.66), P = 0.02, n = 97.
Conclusion: Childhood antibiotic exposure for acute RTI may be a good predictor for subsequent response failure (but not necessarily because of antibiotic treatment failure). Further research is needed to improve understanding of the mechanisms underlying response failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


