{"title":"无症状和轻度症状新冠肺炎患者隔离策略的成本效益分析。","authors":"Unyaporn Suthutvoravut, Patratorn Kunakorntham, Anchisatha Semayai, Amarit Tansawet, Oraluck Pattanaprateep, Pongsathorn Piebpien, Pawin Numthavaj, Ammarin Thakkinstian, Pongsakorn Atiksawedparit","doi":"10.1186/s12962-023-00497-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of COVID-19 patients with mild and moderate symptoms could be isolated at home isolation (HI), community isolation (CI) or hospitel. However, it was still unclear which strategy was more cost-effective. Therefore, this study was conducted to evaluate this.</p><p><strong>Methods: </strong>This study used data from patients who initially stayed at HI, CI, and hospitel under supervision of Ramathibodi Hospital between April and October 2021. Outcomes of interest were hospitalisation and mortality. An incremental cost-effectiveness ratios (ICER) was calculated based on hospital perspective using home isolation as the reference.</p><p><strong>Results: </strong>From 7,077 patients, 4,349 2,356, and 372 were admitted at hospitel, HI, and CI, respectively. Most patients were females (57.04%) and the mean age was 40.42 (SD = 16.15). Average durations of stay were 4.47, 3.35, and 3.91 days for HI, CI, and hospitel, respectively. The average cost per day for staying in these corresponding places were 24.22, 63.69, and 65.23 US$. For hospitalisation, the ICER for hospitel was at 41.93 US$ to avoid one hospitalisation in 1,000 patients when compared to HI, while CI had more cost, but less cases avoided. The ICER for hospitel and CI were at 46.21 and 866.17 US$ to avoid one death in 1,000 patients.</p><p><strong>Conclusions: </strong>HI may be cost-effective isolated strategy for preventing hospitalisation and death in developing countries with limited resources.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"21 1","pages":"85"},"PeriodicalIF":2.5000,"publicationDate":"2023-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10636943/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness analysis of isolation strategies for asymptomatic and mild symptom COVID-19 patients.\",\"authors\":\"Unyaporn Suthutvoravut, Patratorn Kunakorntham, Anchisatha Semayai, Amarit Tansawet, Oraluck Pattanaprateep, Pongsathorn Piebpien, Pawin Numthavaj, Ammarin Thakkinstian, Pongsakorn Atiksawedparit\",\"doi\":\"10.1186/s12962-023-00497-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Management of COVID-19 patients with mild and moderate symptoms could be isolated at home isolation (HI), community isolation (CI) or hospitel. However, it was still unclear which strategy was more cost-effective. Therefore, this study was conducted to evaluate this.</p><p><strong>Methods: </strong>This study used data from patients who initially stayed at HI, CI, and hospitel under supervision of Ramathibodi Hospital between April and October 2021. Outcomes of interest were hospitalisation and mortality. An incremental cost-effectiveness ratios (ICER) was calculated based on hospital perspective using home isolation as the reference.</p><p><strong>Results: </strong>From 7,077 patients, 4,349 2,356, and 372 were admitted at hospitel, HI, and CI, respectively. Most patients were females (57.04%) and the mean age was 40.42 (SD = 16.15). Average durations of stay were 4.47, 3.35, and 3.91 days for HI, CI, and hospitel, respectively. The average cost per day for staying in these corresponding places were 24.22, 63.69, and 65.23 US$. For hospitalisation, the ICER for hospitel was at 41.93 US$ to avoid one hospitalisation in 1,000 patients when compared to HI, while CI had more cost, but less cases avoided. The ICER for hospitel and CI were at 46.21 and 866.17 US$ to avoid one death in 1,000 patients.</p><p><strong>Conclusions: </strong>HI may be cost-effective isolated strategy for preventing hospitalisation and death in developing countries with limited resources.</p>\",\"PeriodicalId\":47054,\"journal\":{\"name\":\"Cost Effectiveness and Resource Allocation\",\"volume\":\"21 1\",\"pages\":\"85\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-11-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10636943/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cost Effectiveness and Resource Allocation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12962-023-00497-x\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-023-00497-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Cost-effectiveness analysis of isolation strategies for asymptomatic and mild symptom COVID-19 patients.
Background: Management of COVID-19 patients with mild and moderate symptoms could be isolated at home isolation (HI), community isolation (CI) or hospitel. However, it was still unclear which strategy was more cost-effective. Therefore, this study was conducted to evaluate this.
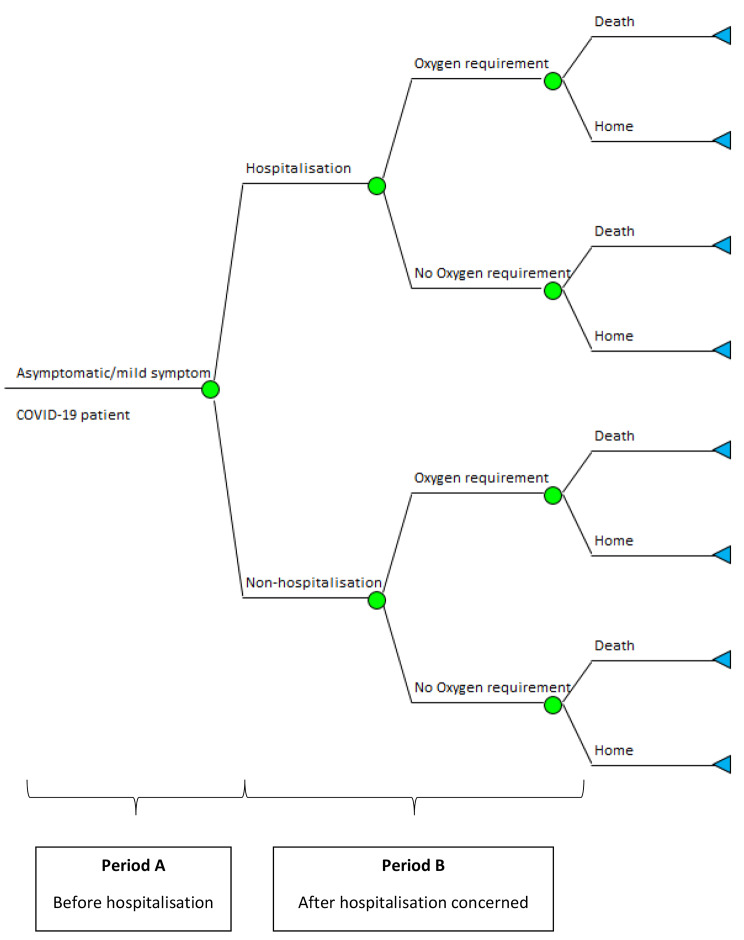
Methods: This study used data from patients who initially stayed at HI, CI, and hospitel under supervision of Ramathibodi Hospital between April and October 2021. Outcomes of interest were hospitalisation and mortality. An incremental cost-effectiveness ratios (ICER) was calculated based on hospital perspective using home isolation as the reference.
Results: From 7,077 patients, 4,349 2,356, and 372 were admitted at hospitel, HI, and CI, respectively. Most patients were females (57.04%) and the mean age was 40.42 (SD = 16.15). Average durations of stay were 4.47, 3.35, and 3.91 days for HI, CI, and hospitel, respectively. The average cost per day for staying in these corresponding places were 24.22, 63.69, and 65.23 US$. For hospitalisation, the ICER for hospitel was at 41.93 US$ to avoid one hospitalisation in 1,000 patients when compared to HI, while CI had more cost, but less cases avoided. The ICER for hospitel and CI were at 46.21 and 866.17 US$ to avoid one death in 1,000 patients.
Conclusions: HI may be cost-effective isolated strategy for preventing hospitalisation and death in developing countries with limited resources.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


