{"title":"一例在直接口服抗凝药物期间使用颅内压监测进行出血性脑梗死两阶段手术的病例。","authors":"Tatsuya Tanaka, Xuan Liu, Nobuaki Momozaki, Eiichiro Honda, Eiichi Suehiro, Akira Matsuno","doi":"10.31662/jmaj.2023-0087","DOIUrl":null,"url":null,"abstract":"<p><p>Direct oral anticoagulants (DOACs) are considered to cause a few hemorrhagic complications, including hemorrhagic infarction; these are administered in the acute phase of cerebral infarction for secondary prevention of cerebral embolism. Hemorrhagic infarction with cerebral herniation requires urgent decompressive craniectomy and can become fatal. Perioperative management is challenging because patients are often on antithrombotic therapy. In this study, we report on a case of a 61-year-old man with left-sided hemiparesis and impaired consciousness; he suffered from a hemorrhagic infarction with cerebral herniation during oral DOAC treatment after endovascular recanalization for the middle cerebral artery occlusion. As the patient was on apixaban for <3 h, performing decompressive craniectomy was considered difficult to stop hemostasis. We then opted to perform a small craniotomy to remove the hematoma, control the intracranial pressure (ICP), and administer fresh frozen plasma. We waited for the effect of apixaban to diminish before performing decompressive craniectomy. Gradually, his level of consciousness was noted to improve. Hemorrhagic cerebral infarction while on DOAC medications can be safely treated with small craniotomy and ICP monitoring followed by decompressive craniectomy. Thus, this case highlights the value of staged surgery under ICP monitoring in the absence of an immediate administration of DOAC antagonists.</p>","PeriodicalId":73550,"journal":{"name":"JMA journal","volume":null,"pages":null},"PeriodicalIF":1.5000,"publicationDate":"2023-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10627977/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Case of Two-stage Surgery Using Intracranial Pressure Monitoring for Hemorrhagic Infarction during Direct Oral Anticoagulant Medication.\",\"authors\":\"Tatsuya Tanaka, Xuan Liu, Nobuaki Momozaki, Eiichiro Honda, Eiichi Suehiro, Akira Matsuno\",\"doi\":\"10.31662/jmaj.2023-0087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Direct oral anticoagulants (DOACs) are considered to cause a few hemorrhagic complications, including hemorrhagic infarction; these are administered in the acute phase of cerebral infarction for secondary prevention of cerebral embolism. Hemorrhagic infarction with cerebral herniation requires urgent decompressive craniectomy and can become fatal. Perioperative management is challenging because patients are often on antithrombotic therapy. In this study, we report on a case of a 61-year-old man with left-sided hemiparesis and impaired consciousness; he suffered from a hemorrhagic infarction with cerebral herniation during oral DOAC treatment after endovascular recanalization for the middle cerebral artery occlusion. As the patient was on apixaban for <3 h, performing decompressive craniectomy was considered difficult to stop hemostasis. We then opted to perform a small craniotomy to remove the hematoma, control the intracranial pressure (ICP), and administer fresh frozen plasma. We waited for the effect of apixaban to diminish before performing decompressive craniectomy. Gradually, his level of consciousness was noted to improve. Hemorrhagic cerebral infarction while on DOAC medications can be safely treated with small craniotomy and ICP monitoring followed by decompressive craniectomy. Thus, this case highlights the value of staged surgery under ICP monitoring in the absence of an immediate administration of DOAC antagonists.</p>\",\"PeriodicalId\":73550,\"journal\":{\"name\":\"JMA journal\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-10-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10627977/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMA journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31662/jmaj.2023-0087\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMA journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31662/jmaj.2023-0087","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
A Case of Two-stage Surgery Using Intracranial Pressure Monitoring for Hemorrhagic Infarction during Direct Oral Anticoagulant Medication.
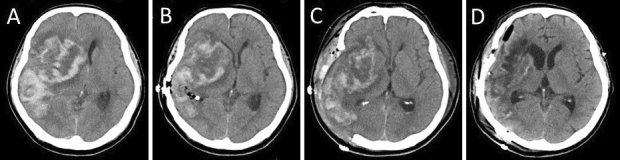
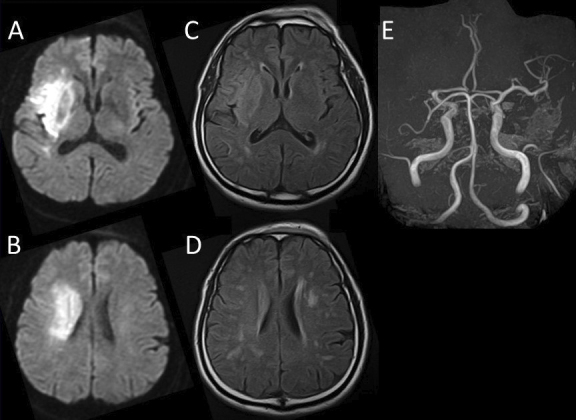
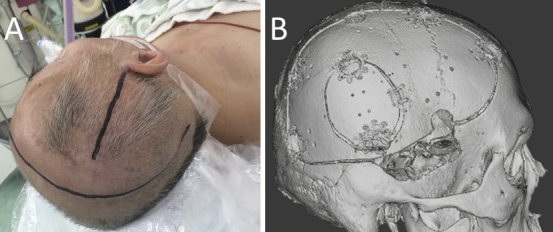
Direct oral anticoagulants (DOACs) are considered to cause a few hemorrhagic complications, including hemorrhagic infarction; these are administered in the acute phase of cerebral infarction for secondary prevention of cerebral embolism. Hemorrhagic infarction with cerebral herniation requires urgent decompressive craniectomy and can become fatal. Perioperative management is challenging because patients are often on antithrombotic therapy. In this study, we report on a case of a 61-year-old man with left-sided hemiparesis and impaired consciousness; he suffered from a hemorrhagic infarction with cerebral herniation during oral DOAC treatment after endovascular recanalization for the middle cerebral artery occlusion. As the patient was on apixaban for <3 h, performing decompressive craniectomy was considered difficult to stop hemostasis. We then opted to perform a small craniotomy to remove the hematoma, control the intracranial pressure (ICP), and administer fresh frozen plasma. We waited for the effect of apixaban to diminish before performing decompressive craniectomy. Gradually, his level of consciousness was noted to improve. Hemorrhagic cerebral infarction while on DOAC medications can be safely treated with small craniotomy and ICP monitoring followed by decompressive craniectomy. Thus, this case highlights the value of staged surgery under ICP monitoring in the absence of an immediate administration of DOAC antagonists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


