Nathaniel J Williams, Joan Russo, Melinda Vredevoogd, Tess Grover, Phillip Green, Enola Proctor, Amritha Bhat, Jürgen Unützer, Ian M Bennett
{"title":"组织文化和氛围与社区卫生中心合作护理孕产妇抑郁症临床结果变化的关系。","authors":"Nathaniel J Williams, Joan Russo, Melinda Vredevoogd, Tess Grover, Phillip Green, Enola Proctor, Amritha Bhat, Jürgen Unützer, Ian M Bennett","doi":"10.1177/26334895231205891","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Organizational factors may help explain variation in the effectiveness of evidence-based clinical innovations through implementation and sustainment. This study tested the relationship between organizational culture and climate and variation in clinical outcomes of the Collaborative Care Model (CoCM) for treatment of maternal depression implemented in community health centers.</p><p><strong>Method: </strong>Organizational cultures and climates of 10 community health centers providing CoCM for depression among low-income women pregnant or parenting were assessed using the organizational social context (OSC) measure. Three-level hierarchical linear models tested whether variation in culture and climate predicted variation in improvement in depression symptoms from baseline to 6.5-month post-baseline for <i>N </i>= 468 women with care ±1 year of OSC assessment. Depression symptomology was measured using the Patient Health Questionnaire (PHQ-9).</p><p><strong>Results: </strong>After controlling for patient characteristics, case mix, center size, and implementation support, patients served by centers with more proficient cultures improved significantly more from baseline to 6.5-month post-baseline than patients in centers with less proficient cultures (mean improvement = 5.08 vs. 0.14, respectively, <i>p</i> = .020), resulting in a large adjusted effect size of <i>d</i><sub>adj</sub> = 0.78. A similar effect was observed for patients served by centers with more functional climates (mean improvement = 5.25 vs. 1.12, <i>p</i> < .044, <i>d</i><sub>adj</sub> = 0.65). Growth models indicated that patients from all centers recovered on average after 4 months of care. However, those with more proficient cultures remained stabilized whereas patients served by centers with less proficient cultures deteriorated by 6.5-month post-baseline. A similar pattern was observed for functional climate.</p><p><strong>Conclusions: </strong>Variation in clinical outcomes for women from historically underserved populations receiving <i>Collaborative Care</i> for maternal depression was associated with the organizational cultures and climates of community health centers. Implementation strategies targeting culture and climate may improve the implementation and effectiveness of integrated behavioral health care for depression.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"4 ","pages":"26334895231205891"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10576428/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of organizational culture and climate with variation in the clinical outcomes of collaborative care for maternal depression in community health centers.\",\"authors\":\"Nathaniel J Williams, Joan Russo, Melinda Vredevoogd, Tess Grover, Phillip Green, Enola Proctor, Amritha Bhat, Jürgen Unützer, Ian M Bennett\",\"doi\":\"10.1177/26334895231205891\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Organizational factors may help explain variation in the effectiveness of evidence-based clinical innovations through implementation and sustainment. This study tested the relationship between organizational culture and climate and variation in clinical outcomes of the Collaborative Care Model (CoCM) for treatment of maternal depression implemented in community health centers.</p><p><strong>Method: </strong>Organizational cultures and climates of 10 community health centers providing CoCM for depression among low-income women pregnant or parenting were assessed using the organizational social context (OSC) measure. Three-level hierarchical linear models tested whether variation in culture and climate predicted variation in improvement in depression symptoms from baseline to 6.5-month post-baseline for <i>N </i>= 468 women with care ±1 year of OSC assessment. Depression symptomology was measured using the Patient Health Questionnaire (PHQ-9).</p><p><strong>Results: </strong>After controlling for patient characteristics, case mix, center size, and implementation support, patients served by centers with more proficient cultures improved significantly more from baseline to 6.5-month post-baseline than patients in centers with less proficient cultures (mean improvement = 5.08 vs. 0.14, respectively, <i>p</i> = .020), resulting in a large adjusted effect size of <i>d</i><sub>adj</sub> = 0.78. A similar effect was observed for patients served by centers with more functional climates (mean improvement = 5.25 vs. 1.12, <i>p</i> < .044, <i>d</i><sub>adj</sub> = 0.65). Growth models indicated that patients from all centers recovered on average after 4 months of care. However, those with more proficient cultures remained stabilized whereas patients served by centers with less proficient cultures deteriorated by 6.5-month post-baseline. A similar pattern was observed for functional climate.</p><p><strong>Conclusions: </strong>Variation in clinical outcomes for women from historically underserved populations receiving <i>Collaborative Care</i> for maternal depression was associated with the organizational cultures and climates of community health centers. Implementation strategies targeting culture and climate may improve the implementation and effectiveness of integrated behavioral health care for depression.</p>\",\"PeriodicalId\":73354,\"journal\":{\"name\":\"Implementation research and practice\",\"volume\":\"4 \",\"pages\":\"26334895231205891\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-10-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10576428/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26334895231205891\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895231205891","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Association of organizational culture and climate with variation in the clinical outcomes of collaborative care for maternal depression in community health centers.
Background: Organizational factors may help explain variation in the effectiveness of evidence-based clinical innovations through implementation and sustainment. This study tested the relationship between organizational culture and climate and variation in clinical outcomes of the Collaborative Care Model (CoCM) for treatment of maternal depression implemented in community health centers.
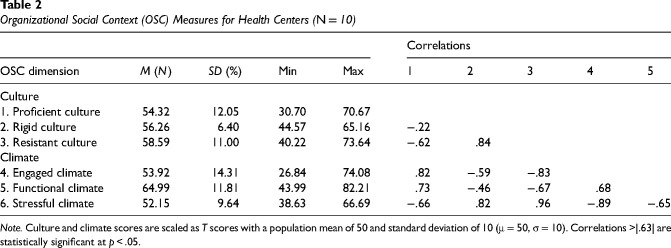
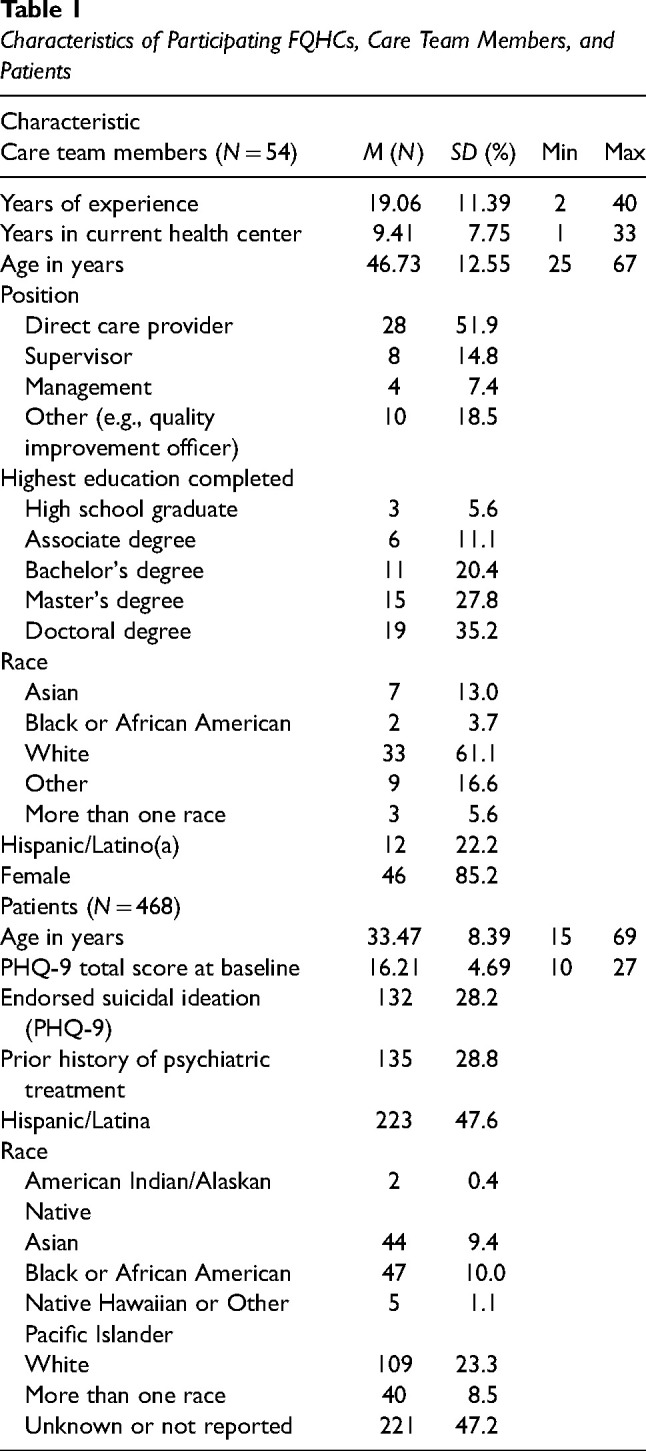
Method: Organizational cultures and climates of 10 community health centers providing CoCM for depression among low-income women pregnant or parenting were assessed using the organizational social context (OSC) measure. Three-level hierarchical linear models tested whether variation in culture and climate predicted variation in improvement in depression symptoms from baseline to 6.5-month post-baseline for N = 468 women with care ±1 year of OSC assessment. Depression symptomology was measured using the Patient Health Questionnaire (PHQ-9).
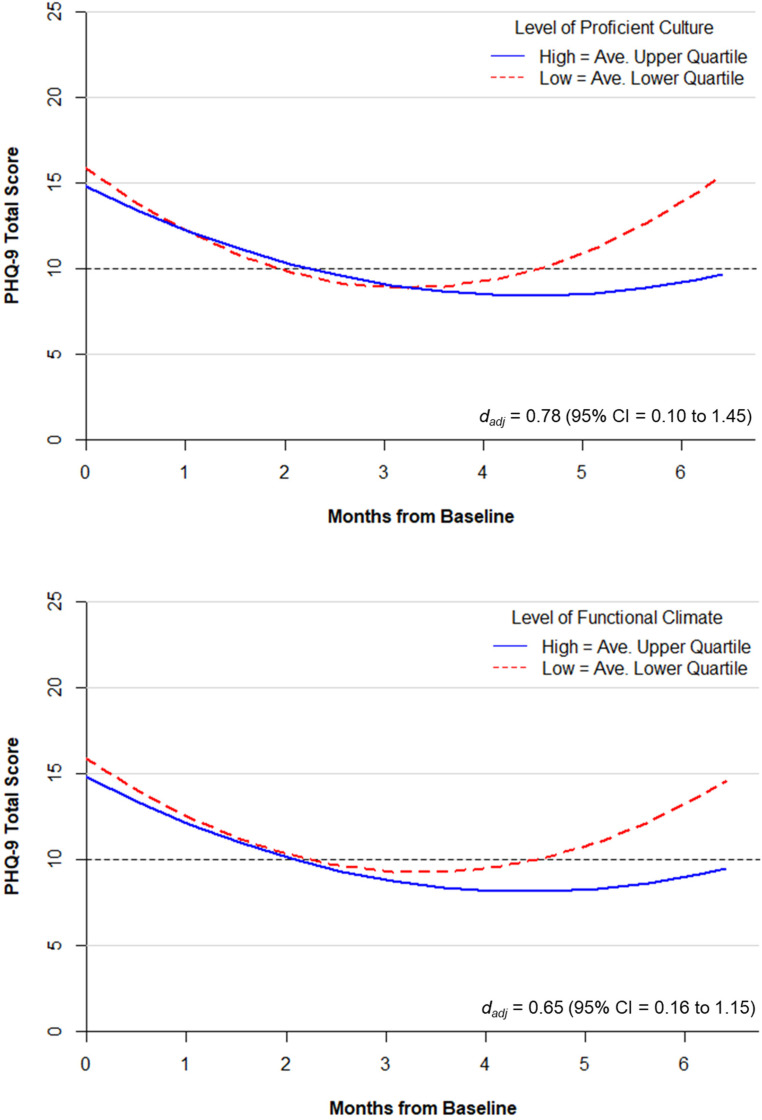
Results: After controlling for patient characteristics, case mix, center size, and implementation support, patients served by centers with more proficient cultures improved significantly more from baseline to 6.5-month post-baseline than patients in centers with less proficient cultures (mean improvement = 5.08 vs. 0.14, respectively, p = .020), resulting in a large adjusted effect size of dadj = 0.78. A similar effect was observed for patients served by centers with more functional climates (mean improvement = 5.25 vs. 1.12, p < .044, dadj = 0.65). Growth models indicated that patients from all centers recovered on average after 4 months of care. However, those with more proficient cultures remained stabilized whereas patients served by centers with less proficient cultures deteriorated by 6.5-month post-baseline. A similar pattern was observed for functional climate.
Conclusions: Variation in clinical outcomes for women from historically underserved populations receiving Collaborative Care for maternal depression was associated with the organizational cultures and climates of community health centers. Implementation strategies targeting culture and climate may improve the implementation and effectiveness of integrated behavioral health care for depression.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


