{"title":"基于药物监测的抗生素治疗方案对危重患者的疗效:随机对照试验的系统综述和荟萃分析。","authors":"Nozomi Takahashi, Yutaka Kondo, Kenji Kubo, Moritoki Egi, Ken-Ichi Kano, Yoshiyasu Ohshima, Taka-Aki Nakada","doi":"10.1186/s40560-023-00699-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The efficacy of therapeutic drug monitoring (TDM)-based antimicrobial dosing optimization strategies on pharmacokinetics/pharmacodynamics and specific drug properties for critically ill patients is unclear. Here, we conducted a systematic review and meta-analysis of randomized controlled trials to evaluate the effectiveness of TDM-based regimen in these patients.</p><p><strong>Methods: </strong>Articles from three databases were systematically retrieved to identify relevant randomized control studies. Version two of the Cochrane tool for assessing risk of bias in randomized trials was used to assess the risk of bias in studies included in the analysis, and quality assessment of evidence was graded using the Grading of Recommendations Assessment, Development, and Evaluation approach. Primary outcome was the 28-day mortality and secondary outcome were in-hospital mortality, clinical cure, length of stay in the intensive care unit (ICU) and target attainment at day 1 and 3.</p><p><strong>Results: </strong>In total, 5 studies involving 1011 patients were included for meta-analysis of the primary outcome, of which no significant difference was observed between TDM-based regimen and control groups (risk ratio [RR] 0.94, 95% confidence interval [CI]: 0.77-1.14; I<sup>2</sup> = 0%). In-hospital mortality (RR 0.96, 95% CI: 0.76-1.20), clinical cure (RR 1.23, 95% CI: 0.91-1.67), length of stay in the ICU (mean difference 0, 95% CI: - 2.18-2.19), and target attainment at day 1 (RR 1.14, 95% CI: 0.88-1.48) and day 3 (RR 1.35, 95% CI: 0.90-2.03) were not significantly different between the two groups, and all evidence for the secondary outcomes had a low or very low level of certainty because the included studies had serious risk of bias, variation of definition for outcomes, and small sample sizes.</p><p><strong>Conclusion: </strong>TDM-based regimens had no significant efficacy for clinical or pharmacological outcomes. Further studies with other achievable targets and well-defined outcomes are required.</p><p><strong>Trial registration: </strong>Clinical trial registration; PROSPERO ( https://www.crd.york.ac.uk/prospero/ ), registry number: CRD 42022371959. Registered 24 November 2022.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"48"},"PeriodicalIF":4.7000,"publicationDate":"2023-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631080/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy of therapeutic drug monitoring-based antibiotic regimen in critically ill patients: a systematic review and meta-analysis of randomized controlled trials.\",\"authors\":\"Nozomi Takahashi, Yutaka Kondo, Kenji Kubo, Moritoki Egi, Ken-Ichi Kano, Yoshiyasu Ohshima, Taka-Aki Nakada\",\"doi\":\"10.1186/s40560-023-00699-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The efficacy of therapeutic drug monitoring (TDM)-based antimicrobial dosing optimization strategies on pharmacokinetics/pharmacodynamics and specific drug properties for critically ill patients is unclear. Here, we conducted a systematic review and meta-analysis of randomized controlled trials to evaluate the effectiveness of TDM-based regimen in these patients.</p><p><strong>Methods: </strong>Articles from three databases were systematically retrieved to identify relevant randomized control studies. Version two of the Cochrane tool for assessing risk of bias in randomized trials was used to assess the risk of bias in studies included in the analysis, and quality assessment of evidence was graded using the Grading of Recommendations Assessment, Development, and Evaluation approach. Primary outcome was the 28-day mortality and secondary outcome were in-hospital mortality, clinical cure, length of stay in the intensive care unit (ICU) and target attainment at day 1 and 3.</p><p><strong>Results: </strong>In total, 5 studies involving 1011 patients were included for meta-analysis of the primary outcome, of which no significant difference was observed between TDM-based regimen and control groups (risk ratio [RR] 0.94, 95% confidence interval [CI]: 0.77-1.14; I<sup>2</sup> = 0%). In-hospital mortality (RR 0.96, 95% CI: 0.76-1.20), clinical cure (RR 1.23, 95% CI: 0.91-1.67), length of stay in the ICU (mean difference 0, 95% CI: - 2.18-2.19), and target attainment at day 1 (RR 1.14, 95% CI: 0.88-1.48) and day 3 (RR 1.35, 95% CI: 0.90-2.03) were not significantly different between the two groups, and all evidence for the secondary outcomes had a low or very low level of certainty because the included studies had serious risk of bias, variation of definition for outcomes, and small sample sizes.</p><p><strong>Conclusion: </strong>TDM-based regimens had no significant efficacy for clinical or pharmacological outcomes. Further studies with other achievable targets and well-defined outcomes are required.</p><p><strong>Trial registration: </strong>Clinical trial registration; PROSPERO ( https://www.crd.york.ac.uk/prospero/ ), registry number: CRD 42022371959. Registered 24 November 2022.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"11 1\",\"pages\":\"48\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-11-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631080/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00699-8\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00699-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Efficacy of therapeutic drug monitoring-based antibiotic regimen in critically ill patients: a systematic review and meta-analysis of randomized controlled trials.
Background: The efficacy of therapeutic drug monitoring (TDM)-based antimicrobial dosing optimization strategies on pharmacokinetics/pharmacodynamics and specific drug properties for critically ill patients is unclear. Here, we conducted a systematic review and meta-analysis of randomized controlled trials to evaluate the effectiveness of TDM-based regimen in these patients.
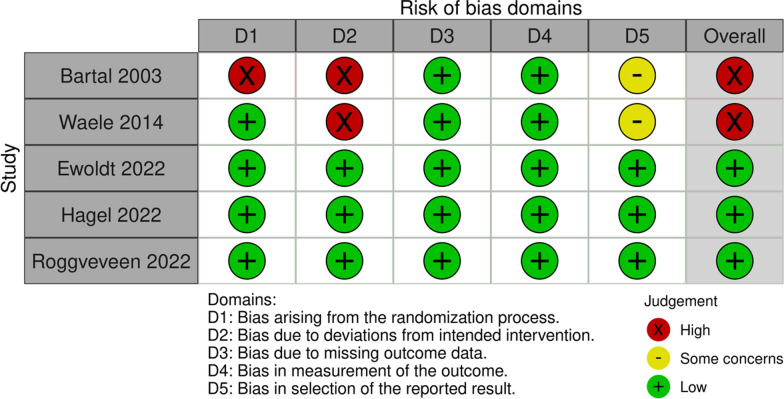
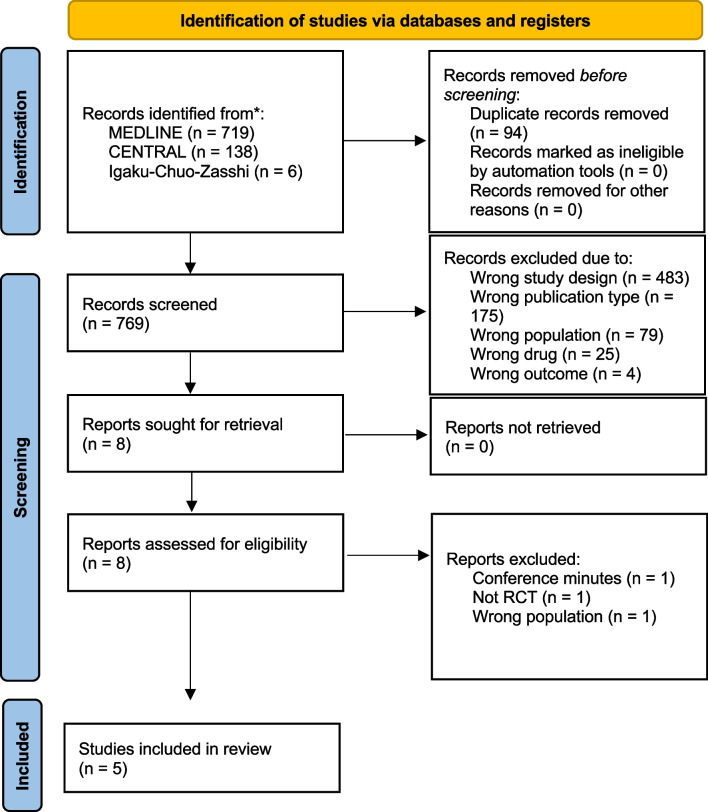
Methods: Articles from three databases were systematically retrieved to identify relevant randomized control studies. Version two of the Cochrane tool for assessing risk of bias in randomized trials was used to assess the risk of bias in studies included in the analysis, and quality assessment of evidence was graded using the Grading of Recommendations Assessment, Development, and Evaluation approach. Primary outcome was the 28-day mortality and secondary outcome were in-hospital mortality, clinical cure, length of stay in the intensive care unit (ICU) and target attainment at day 1 and 3.
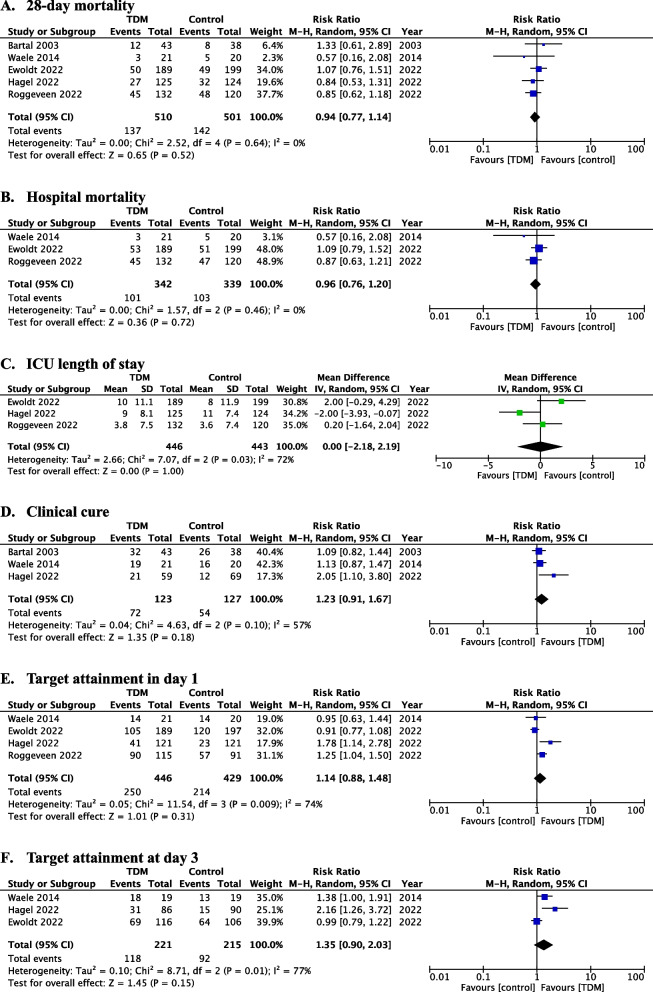
Results: In total, 5 studies involving 1011 patients were included for meta-analysis of the primary outcome, of which no significant difference was observed between TDM-based regimen and control groups (risk ratio [RR] 0.94, 95% confidence interval [CI]: 0.77-1.14; I2 = 0%). In-hospital mortality (RR 0.96, 95% CI: 0.76-1.20), clinical cure (RR 1.23, 95% CI: 0.91-1.67), length of stay in the ICU (mean difference 0, 95% CI: - 2.18-2.19), and target attainment at day 1 (RR 1.14, 95% CI: 0.88-1.48) and day 3 (RR 1.35, 95% CI: 0.90-2.03) were not significantly different between the two groups, and all evidence for the secondary outcomes had a low or very low level of certainty because the included studies had serious risk of bias, variation of definition for outcomes, and small sample sizes.
Conclusion: TDM-based regimens had no significant efficacy for clinical or pharmacological outcomes. Further studies with other achievable targets and well-defined outcomes are required.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


