Jessica L. Beadle, Sarah M. Perman, Justin Pennington, David F. Gaieski
{"title":"急诊科入院败血症患者体温和发热负担的调查","authors":"Jessica L. Beadle, Sarah M. Perman, Justin Pennington, David F. Gaieski","doi":"10.1002/ams2.902","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>We sought to collect granular data on temperature burden to further explore existing conflicting information on the relationship between temperature alterations and outcomes in patients with sepsis requiring hospital admission.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a prospective cohort study that enrolled a convenience sample of patients with sepsis or septic shock admitted to the hospital from the emergency department (ED). A “unit of temperature burden (UTB)” was defined as >1°C (1.8°F) above or below 37°C (98.6°F) for 1 min. Fever burden was defined as the number of UTBs >38°C (100.4°F). The primary objective was to calculate the fever burden in patients with sepsis during their ED stay. This was analyzed for patients who present to triage febrile or hypothermic and also for those who developed temperature abnormalities during their ED stay. The secondary objectives were correlating fever and hypothermia burden with in-hospital mortality, Systemic Inflammatory Response Syndrome (SIRS) criteria, and the quick Sequential (Sepsis-Associated) Organ Failure Assessment (qSOFA) score and identification of patients who may benefit from early implementation of targeted temperature management.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 256 patients met the inclusion criteria. The mean age of patients was 60.1 ± 18.4 years; 46% were female and 29.6% were black. The median (interquartile range [IQR]) fever burden for the fever in triage cohort (<i>n</i> = 99) was 364.6 (174.3-716.8) UTB and for the no fever in triage cohort (<i>n</i> = 157) was 179.3 (80.9-374.0) UTB (p = 0.005). The two groups had similar in-hospital mortality (6.1 vs 8.3%; p = 0.5). The median fever burden for the fever anytime cohort was 303.8 (IQR 138.8-607.9) UTB and they had lower mortality than the no fever anytime cohort (4.7% vs 11.2%; p = 0.052). Patients with fever at triage had higher mean SIRS criteria than those without (2.8 vs 2.0; p < 0.001) while qSOFA points were similar (p = 0.199). A total of 27 patients had hypothermia during their ED stay and these patients were older with higher mean SIRS criteria.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Patients with sepsis and septic shock have a significant temperature burden in the ED. When comparing patients who had fever at any time during their ED stay with those who never had a fever, a trend toward an inverse relationship between fever burden and mortality was found.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"10 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2023-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10622605/pdf/","citationCount":"0","resultStr":"{\"title\":\"An investigation of temperature and fever burdens in patients with sepsis admitted from the emergency department to the hospital\",\"authors\":\"Jessica L. Beadle, Sarah M. Perman, Justin Pennington, David F. Gaieski\",\"doi\":\"10.1002/ams2.902\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>We sought to collect granular data on temperature burden to further explore existing conflicting information on the relationship between temperature alterations and outcomes in patients with sepsis requiring hospital admission.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a prospective cohort study that enrolled a convenience sample of patients with sepsis or septic shock admitted to the hospital from the emergency department (ED). A “unit of temperature burden (UTB)” was defined as >1°C (1.8°F) above or below 37°C (98.6°F) for 1 min. Fever burden was defined as the number of UTBs >38°C (100.4°F). The primary objective was to calculate the fever burden in patients with sepsis during their ED stay. This was analyzed for patients who present to triage febrile or hypothermic and also for those who developed temperature abnormalities during their ED stay. The secondary objectives were correlating fever and hypothermia burden with in-hospital mortality, Systemic Inflammatory Response Syndrome (SIRS) criteria, and the quick Sequential (Sepsis-Associated) Organ Failure Assessment (qSOFA) score and identification of patients who may benefit from early implementation of targeted temperature management.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 256 patients met the inclusion criteria. The mean age of patients was 60.1 ± 18.4 years; 46% were female and 29.6% were black. The median (interquartile range [IQR]) fever burden for the fever in triage cohort (<i>n</i> = 99) was 364.6 (174.3-716.8) UTB and for the no fever in triage cohort (<i>n</i> = 157) was 179.3 (80.9-374.0) UTB (p = 0.005). The two groups had similar in-hospital mortality (6.1 vs 8.3%; p = 0.5). The median fever burden for the fever anytime cohort was 303.8 (IQR 138.8-607.9) UTB and they had lower mortality than the no fever anytime cohort (4.7% vs 11.2%; p = 0.052). Patients with fever at triage had higher mean SIRS criteria than those without (2.8 vs 2.0; p < 0.001) while qSOFA points were similar (p = 0.199). A total of 27 patients had hypothermia during their ED stay and these patients were older with higher mean SIRS criteria.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Patients with sepsis and septic shock have a significant temperature burden in the ED. When comparing patients who had fever at any time during their ED stay with those who never had a fever, a trend toward an inverse relationship between fever burden and mortality was found.</p>\\n </section>\\n </div>\",\"PeriodicalId\":7196,\"journal\":{\"name\":\"Acute Medicine & Surgery\",\"volume\":\"10 1\",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-11-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10622605/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute Medicine & Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ams2.902\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.902","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的:我们试图收集关于温度负担的颗粒数据,以进一步探索需要住院的败血症患者温度变化与预后之间关系的现有相互矛盾的信息。方法:这是一项前瞻性队列研究,纳入了从急诊科(ED)入院的脓毒症或感染性休克患者的方便样本。“温度负荷单位(UTB)”定义为高于或低于37°C(98.6°F) 1分钟1°C(1.8°F)。发热负担定义为38°C(100.4°F)的utb数量。主要目的是计算败血症患者在急诊科住院期间的发热负担。分析了出现发热或体温过低的患者以及在急诊科住院期间出现体温异常的患者。次要目标是将发热和低温负担与住院死亡率、全身炎症反应综合征(SIRS)标准、快速序事性(败血症相关)器官衰竭评估(qSOFA)评分以及确定可能从早期实施靶向温度管理中受益的患者之间的关系。结果256例患者符合纳入标准。患者平均年龄60.1±18.4岁;46%为女性,29.6%为黑人。分诊组发热组(n = 99)发热负荷中位数(四分位间距[IQR])为364.6 (174.3-716.8)UTB,无发热组(n = 157)发热负荷中位数(80.9-374.0)UTB (p = 0.005)。两组的住院死亡率相似(6.1% vs 8.3%;p = 0.5)。随时发烧组的中位发烧负担为303.8 (IQR 138.8-607.9) UTB,死亡率低于随时不发烧组(4.7% vs 11.2%;p = 0.052)。分诊时发烧的患者比没有发烧的患者有更高的SIRS平均标准(2.8 vs 2.0;p < 0.001),而qSOFA积分相似(p = 0.199)。共有27例患者在急诊科住院期间发生低温症,这些患者年龄较大,平均SIRS标准较高。结论脓毒症和脓毒性休克患者在急诊科有明显的温度负担。通过比较在急诊科住院期间任何时间发烧的患者与从未发烧的患者,发现发烧负担与死亡率呈反比关系。
An investigation of temperature and fever burdens in patients with sepsis admitted from the emergency department to the hospital
Aim
We sought to collect granular data on temperature burden to further explore existing conflicting information on the relationship between temperature alterations and outcomes in patients with sepsis requiring hospital admission.
Methods
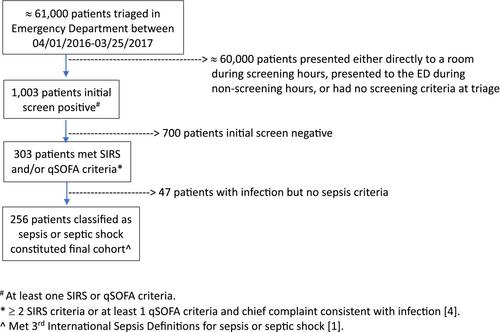
This was a prospective cohort study that enrolled a convenience sample of patients with sepsis or septic shock admitted to the hospital from the emergency department (ED). A “unit of temperature burden (UTB)” was defined as >1°C (1.8°F) above or below 37°C (98.6°F) for 1 min. Fever burden was defined as the number of UTBs >38°C (100.4°F). The primary objective was to calculate the fever burden in patients with sepsis during their ED stay. This was analyzed for patients who present to triage febrile or hypothermic and also for those who developed temperature abnormalities during their ED stay. The secondary objectives were correlating fever and hypothermia burden with in-hospital mortality, Systemic Inflammatory Response Syndrome (SIRS) criteria, and the quick Sequential (Sepsis-Associated) Organ Failure Assessment (qSOFA) score and identification of patients who may benefit from early implementation of targeted temperature management.
Results
A total of 256 patients met the inclusion criteria. The mean age of patients was 60.1 ± 18.4 years; 46% were female and 29.6% were black. The median (interquartile range [IQR]) fever burden for the fever in triage cohort (n = 99) was 364.6 (174.3-716.8) UTB and for the no fever in triage cohort (n = 157) was 179.3 (80.9-374.0) UTB (p = 0.005). The two groups had similar in-hospital mortality (6.1 vs 8.3%; p = 0.5). The median fever burden for the fever anytime cohort was 303.8 (IQR 138.8-607.9) UTB and they had lower mortality than the no fever anytime cohort (4.7% vs 11.2%; p = 0.052). Patients with fever at triage had higher mean SIRS criteria than those without (2.8 vs 2.0; p < 0.001) while qSOFA points were similar (p = 0.199). A total of 27 patients had hypothermia during their ED stay and these patients were older with higher mean SIRS criteria.
Conclusions
Patients with sepsis and septic shock have a significant temperature burden in the ED. When comparing patients who had fever at any time during their ED stay with those who never had a fever, a trend toward an inverse relationship between fever burden and mortality was found.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


