{"title":"富有同情心的社区连接器计划:对医疗保健使用的影响。","authors":"Samar M Aoun, Natasha Bear, Bruce Rumbold","doi":"10.1177/26323524231205323","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Public health approaches to palliative and end-of-life care focus on enhancing the integration of services and providing a comprehensive approach that engages the assets of local communities. However, few studies have evaluated the relative costs and benefits of providing care using these service models.</p><p><strong>Objectives: </strong>To assess the effect on healthcare usage of a community-based palliative care program ('Compassionate Communities Connectors') where practical and social support was delivered by community volunteers to people living with advanced life-limiting illnesses in regional Western Australia.</p><p><strong>Design: </strong>Controlled before-and-after study/Cost-consequence analysis.</p><p><strong>Methods: </strong>A total of 43 community-based patients participated in the program during the period 2020-2022. A comparator population of 172 individuals with advanced life-limiting illnesses was randomly selected from usage data from the same set of health services.</p><p><strong>Results: </strong>Relative to controls, the intervention group had lower hospitalizations per month [Incidence rate ratio (IRR): 0.37; 95% CI: 0.18-0.77, <i>p</i> = 0.007], less hospital days per month (IRR: 0.23; 95% CI: 0.11-0.49, <i>p</i> < 0.001) and less emergency presentations (IRR: 0.56; 95% CI: 0.34-0.94, <i>p</i> = 0.028. The frequency of outpatient contacts overall was two times higher for the intervention group (IRR: 2.07; 95% CI: 1.11-3.86, <i>p</i> = 0.022), indicating the Connector program may have shifted individuals away from the hospital system and toward community-based care. Estimated net savings of $AUD 518,701 would be achieved from adopting the Connector program, assuming enrollment of 100 patients over an average 6-month participation period.</p><p><strong>Conclusion: </strong>This combined healthcare usage and economic analysis of the 'Compassionate Communities Connectors' program demonstrates the benefits of optimizing palliative care services using home-based and community-centered interventions, with gains for the health system through improved patient outcomes and reduced total healthcare costs (including fewer hospitalizations and readmissions). These findings, coupled with the other published results, suggest that investment in the Connectors program has the capacity to reduce net health sector expenditure while also improving outcomes for people with life-limiting illnesses.</p><p><strong>Trial registration: </strong>Australian and New Zealand Clinical Trial Registry: ACTRN12620000326998.</p>","PeriodicalId":36693,"journal":{"name":"Palliative Care and Social Practice","volume":"17 ","pages":"26323524231205323"},"PeriodicalIF":2.7000,"publicationDate":"2023-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10612440/pdf/","citationCount":"0","resultStr":"{\"title\":\"The compassionate communities connectors program: effect on healthcare usage.\",\"authors\":\"Samar M Aoun, Natasha Bear, Bruce Rumbold\",\"doi\":\"10.1177/26323524231205323\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Public health approaches to palliative and end-of-life care focus on enhancing the integration of services and providing a comprehensive approach that engages the assets of local communities. However, few studies have evaluated the relative costs and benefits of providing care using these service models.</p><p><strong>Objectives: </strong>To assess the effect on healthcare usage of a community-based palliative care program ('Compassionate Communities Connectors') where practical and social support was delivered by community volunteers to people living with advanced life-limiting illnesses in regional Western Australia.</p><p><strong>Design: </strong>Controlled before-and-after study/Cost-consequence analysis.</p><p><strong>Methods: </strong>A total of 43 community-based patients participated in the program during the period 2020-2022. A comparator population of 172 individuals with advanced life-limiting illnesses was randomly selected from usage data from the same set of health services.</p><p><strong>Results: </strong>Relative to controls, the intervention group had lower hospitalizations per month [Incidence rate ratio (IRR): 0.37; 95% CI: 0.18-0.77, <i>p</i> = 0.007], less hospital days per month (IRR: 0.23; 95% CI: 0.11-0.49, <i>p</i> < 0.001) and less emergency presentations (IRR: 0.56; 95% CI: 0.34-0.94, <i>p</i> = 0.028. The frequency of outpatient contacts overall was two times higher for the intervention group (IRR: 2.07; 95% CI: 1.11-3.86, <i>p</i> = 0.022), indicating the Connector program may have shifted individuals away from the hospital system and toward community-based care. Estimated net savings of $AUD 518,701 would be achieved from adopting the Connector program, assuming enrollment of 100 patients over an average 6-month participation period.</p><p><strong>Conclusion: </strong>This combined healthcare usage and economic analysis of the 'Compassionate Communities Connectors' program demonstrates the benefits of optimizing palliative care services using home-based and community-centered interventions, with gains for the health system through improved patient outcomes and reduced total healthcare costs (including fewer hospitalizations and readmissions). These findings, coupled with the other published results, suggest that investment in the Connectors program has the capacity to reduce net health sector expenditure while also improving outcomes for people with life-limiting illnesses.</p><p><strong>Trial registration: </strong>Australian and New Zealand Clinical Trial Registry: ACTRN12620000326998.</p>\",\"PeriodicalId\":36693,\"journal\":{\"name\":\"Palliative Care and Social Practice\",\"volume\":\"17 \",\"pages\":\"26323524231205323\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2023-10-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10612440/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Palliative Care and Social Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26323524231205323\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care and Social Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26323524231205323","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
背景:姑息治疗和临终关怀的公共卫生方法侧重于加强服务的整合,并提供一种吸引当地社区资产的综合方法。然而,很少有研究评估使用这些服务模式提供护理的相对成本和收益。目的:评估社区姑息治疗计划(“同情社区连接器”)对医疗保健使用的影响,该计划由社区志愿者向西澳大利亚地区患有晚期限制生命疾病的人提供实际和社会支持。设计:研究前后对照/成本-后果分析。方法:2020-2022年期间,共有43名社区患者参与了该项目。从同一组卫生服务的使用数据中随机选择了172名患有晚期限制生命疾病的对照人群。结果:与对照组相比,干预组每月住院人数较低[发病率比(IRR):0.37;95%可信区间:0.18-0.77,p = 0.007],每月减少住院天数(内部收益率:0.23;95%置信区间:0.11-0.49,p p = 0.028。干预组的门诊接触频率总体上高出两倍(IRR:2.07;95%CI:1.11-3.86,p = 0.022),表明连接器计划可能已将个人从医院系统转移到社区护理。假设在平均6个月的参与期内有100名患者参与,采用连接器计划预计将实现518701澳元的净节约。结论:“同情社区连接器”计划的医疗保健使用和经济分析相结合,证明了使用基于家庭和以社区为中心的干预措施优化姑息治疗服务的好处,并通过改善患者结果和降低医疗保健总成本(包括减少住院和再次入院)为卫生系统带来收益。这些发现,再加上其他已发表的结果,表明对连接器计划的投资有能力减少卫生部门的净支出,同时也能改善患有限制生命疾病的人的结果。试验注册:澳大利亚和新西兰临床试验注册:ACTRN12620000326998。
The compassionate communities connectors program: effect on healthcare usage.
Background: Public health approaches to palliative and end-of-life care focus on enhancing the integration of services and providing a comprehensive approach that engages the assets of local communities. However, few studies have evaluated the relative costs and benefits of providing care using these service models.
Objectives: To assess the effect on healthcare usage of a community-based palliative care program ('Compassionate Communities Connectors') where practical and social support was delivered by community volunteers to people living with advanced life-limiting illnesses in regional Western Australia.
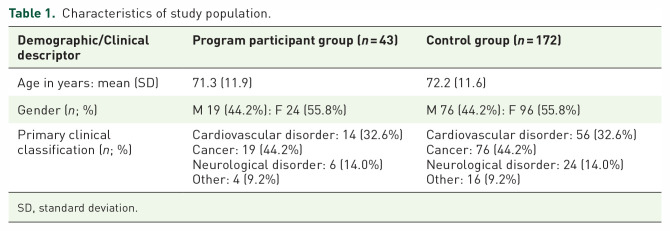
Methods: A total of 43 community-based patients participated in the program during the period 2020-2022. A comparator population of 172 individuals with advanced life-limiting illnesses was randomly selected from usage data from the same set of health services.
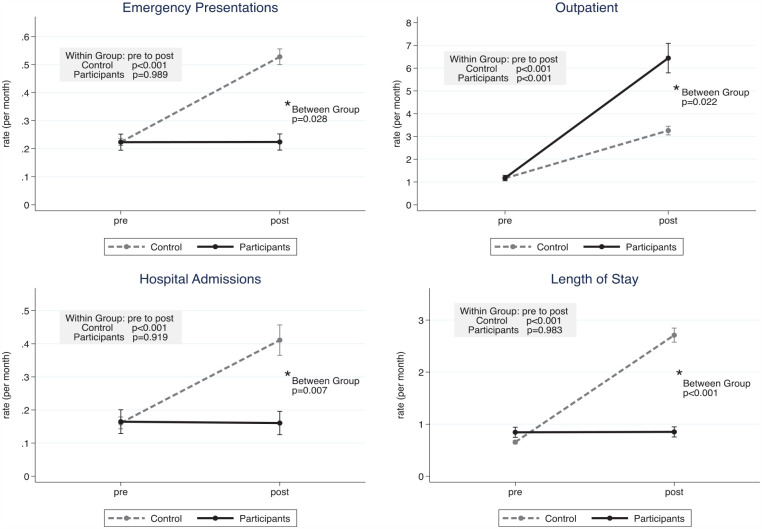
Results: Relative to controls, the intervention group had lower hospitalizations per month [Incidence rate ratio (IRR): 0.37; 95% CI: 0.18-0.77, p = 0.007], less hospital days per month (IRR: 0.23; 95% CI: 0.11-0.49, p < 0.001) and less emergency presentations (IRR: 0.56; 95% CI: 0.34-0.94, p = 0.028. The frequency of outpatient contacts overall was two times higher for the intervention group (IRR: 2.07; 95% CI: 1.11-3.86, p = 0.022), indicating the Connector program may have shifted individuals away from the hospital system and toward community-based care. Estimated net savings of $AUD 518,701 would be achieved from adopting the Connector program, assuming enrollment of 100 patients over an average 6-month participation period.
Conclusion: This combined healthcare usage and economic analysis of the 'Compassionate Communities Connectors' program demonstrates the benefits of optimizing palliative care services using home-based and community-centered interventions, with gains for the health system through improved patient outcomes and reduced total healthcare costs (including fewer hospitalizations and readmissions). These findings, coupled with the other published results, suggest that investment in the Connectors program has the capacity to reduce net health sector expenditure while also improving outcomes for people with life-limiting illnesses.
Trial registration: Australian and New Zealand Clinical Trial Registry: ACTRN12620000326998.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


