Abdo Jurjus , Assad Eid , Sahar Al Kattar , Marie Noel Zeenny , Alice Gerges-Geagea , Hanine Haydar , Anis Hilal , Doreid Oueidat , Michel Matar , Jihane Tawilah , Inaya Hajj Hussein , Pierre Schembri-Wismayer , Francesco Cappello , Giovanni Tomasello , Angelo Leone , Rosalyn A. Jurjus
{"title":"炎症性肠病,结直肠癌癌症和2型糖尿病:联系。","authors":"Abdo Jurjus , Assad Eid , Sahar Al Kattar , Marie Noel Zeenny , Alice Gerges-Geagea , Hanine Haydar , Anis Hilal , Doreid Oueidat , Michel Matar , Jihane Tawilah , Inaya Hajj Hussein , Pierre Schembri-Wismayer , Francesco Cappello , Giovanni Tomasello , Angelo Leone , Rosalyn A. Jurjus","doi":"10.1016/j.bbacli.2015.11.002","DOIUrl":null,"url":null,"abstract":"<div><p>The co-occurrence of the three disease entities, inflammatory bowel disease (IBD), colorectal cancer (CRC), type 2diabetes mellitus (T2DM) along with inflammation and dismicrobism has been frequently reported. Some authors have even suggested that dysbiosis could be the link through a molecular crosstalk of multiple inflammatory loops including TGFβ, NFKB, TNFα and ROS among others.</p><p>This review focuses on the inflammatory process along with the role of microbiota in the pathophysiology of the three diseases.</p><p>The etiology of IBD is multifactorial, and like CRC and T2DM, it is associated with a widespread and sustained GI inflammation and dismicrobism, whereby an array of pro-inflammatory mediators and other related biomolecules are up-regulated, both locally and systematically. Such a persistent or an inadequately resolved chronic inflammation may be a causative agent, in the presence other factors, leading to several pathologies such as IBD, CRC and T2DM.</p><p>TGFβ plays a crucial role in pancreatic β cell malfunctioning as glucotoxicity stimulates its signaling cascade through smad 3, IL-6 and epithelial to mesenchymal transition. Such a cascade could lead to macrophages and other cells recruitment, inflammation, then IBD and CRC.</p><p>NFkB is also another key regulator in the crosstalk among the pathways leading to the three disease entities. It plays a major role in linking inflammation to cancer development through its ability to up regulate several inflammatory and tumor promoting cytokines like: IL-6, IL-1 α and TNF α, as well as genes like BCL2 and BCLXL. It activates JAK/STAT signaling network via STAT3 transcription factors and promotes epithelial to mesenchymal transition. It also increases the risk for T2DM in obese people. In brief, NFKB is a matchmaker between inflammation, IBD, cancer and diabetes.</p><p>In addition, TNFα plays a pivotal role in systemic inflammation. It is increased in the mucosa of IBD patients and has a central role in its pathogenesis. It also activates other signaling pathways like NFKB and MAPK leading to CRC. It is also overexpressed in the adipose tissues of obese patients thus linking it to T2DM, chronic inflammation and consequently CRC.</p><p>On the other hand, increasing evidence suggests that dysbiosis plays a role in initiating, maintaining and determining the severity of IBD. Actually, among its functions, it modulates genotoxic metabolites which are able to induce CRC, a fact proven to be sustained by stool transfer from patients with CRC. Probiotics, however, may actively prevent CRC as well as IBD and results in a significant decrease in fasting glycemia in T2DM patients.</p><p>In conclusion, IBD, CRC and T2DM are commonly occurring interrelated clinical problems. They share a common basis influenced by an inflammatory process, an imbalance in intestinal microbiota, and a crosstalk between various signaling pathways. Would probiotics interrupt the crosstalk or orient it in the physiological direction?</p></div>","PeriodicalId":72344,"journal":{"name":"BBA clinical","volume":"5 ","pages":"Pages 16-24"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.bbacli.2015.11.002","citationCount":"117","resultStr":"{\"title\":\"Inflammatory bowel disease, colorectal cancer and type 2 diabetes mellitus: The links\",\"authors\":\"Abdo Jurjus , Assad Eid , Sahar Al Kattar , Marie Noel Zeenny , Alice Gerges-Geagea , Hanine Haydar , Anis Hilal , Doreid Oueidat , Michel Matar , Jihane Tawilah , Inaya Hajj Hussein , Pierre Schembri-Wismayer , Francesco Cappello , Giovanni Tomasello , Angelo Leone , Rosalyn A. Jurjus\",\"doi\":\"10.1016/j.bbacli.2015.11.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>The co-occurrence of the three disease entities, inflammatory bowel disease (IBD), colorectal cancer (CRC), type 2diabetes mellitus (T2DM) along with inflammation and dismicrobism has been frequently reported. Some authors have even suggested that dysbiosis could be the link through a molecular crosstalk of multiple inflammatory loops including TGFβ, NFKB, TNFα and ROS among others.</p><p>This review focuses on the inflammatory process along with the role of microbiota in the pathophysiology of the three diseases.</p><p>The etiology of IBD is multifactorial, and like CRC and T2DM, it is associated with a widespread and sustained GI inflammation and dismicrobism, whereby an array of pro-inflammatory mediators and other related biomolecules are up-regulated, both locally and systematically. Such a persistent or an inadequately resolved chronic inflammation may be a causative agent, in the presence other factors, leading to several pathologies such as IBD, CRC and T2DM.</p><p>TGFβ plays a crucial role in pancreatic β cell malfunctioning as glucotoxicity stimulates its signaling cascade through smad 3, IL-6 and epithelial to mesenchymal transition. Such a cascade could lead to macrophages and other cells recruitment, inflammation, then IBD and CRC.</p><p>NFkB is also another key regulator in the crosstalk among the pathways leading to the three disease entities. It plays a major role in linking inflammation to cancer development through its ability to up regulate several inflammatory and tumor promoting cytokines like: IL-6, IL-1 α and TNF α, as well as genes like BCL2 and BCLXL. It activates JAK/STAT signaling network via STAT3 transcription factors and promotes epithelial to mesenchymal transition. It also increases the risk for T2DM in obese people. In brief, NFKB is a matchmaker between inflammation, IBD, cancer and diabetes.</p><p>In addition, TNFα plays a pivotal role in systemic inflammation. It is increased in the mucosa of IBD patients and has a central role in its pathogenesis. It also activates other signaling pathways like NFKB and MAPK leading to CRC. It is also overexpressed in the adipose tissues of obese patients thus linking it to T2DM, chronic inflammation and consequently CRC.</p><p>On the other hand, increasing evidence suggests that dysbiosis plays a role in initiating, maintaining and determining the severity of IBD. Actually, among its functions, it modulates genotoxic metabolites which are able to induce CRC, a fact proven to be sustained by stool transfer from patients with CRC. Probiotics, however, may actively prevent CRC as well as IBD and results in a significant decrease in fasting glycemia in T2DM patients.</p><p>In conclusion, IBD, CRC and T2DM are commonly occurring interrelated clinical problems. They share a common basis influenced by an inflammatory process, an imbalance in intestinal microbiota, and a crosstalk between various signaling pathways. Would probiotics interrupt the crosstalk or orient it in the physiological direction?</p></div>\",\"PeriodicalId\":72344,\"journal\":{\"name\":\"BBA clinical\",\"volume\":\"5 \",\"pages\":\"Pages 16-24\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.bbacli.2015.11.002\",\"citationCount\":\"117\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BBA clinical\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2214647415000975\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BBA clinical","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214647415000975","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Inflammatory bowel disease, colorectal cancer and type 2 diabetes mellitus: The links
The co-occurrence of the three disease entities, inflammatory bowel disease (IBD), colorectal cancer (CRC), type 2diabetes mellitus (T2DM) along with inflammation and dismicrobism has been frequently reported. Some authors have even suggested that dysbiosis could be the link through a molecular crosstalk of multiple inflammatory loops including TGFβ, NFKB, TNFα and ROS among others.
This review focuses on the inflammatory process along with the role of microbiota in the pathophysiology of the three diseases.
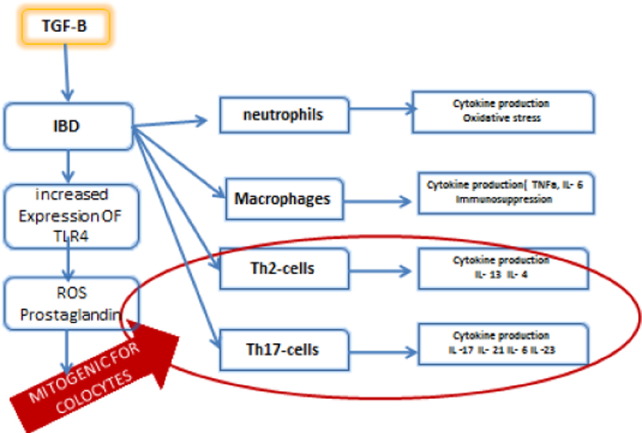
The etiology of IBD is multifactorial, and like CRC and T2DM, it is associated with a widespread and sustained GI inflammation and dismicrobism, whereby an array of pro-inflammatory mediators and other related biomolecules are up-regulated, both locally and systematically. Such a persistent or an inadequately resolved chronic inflammation may be a causative agent, in the presence other factors, leading to several pathologies such as IBD, CRC and T2DM.
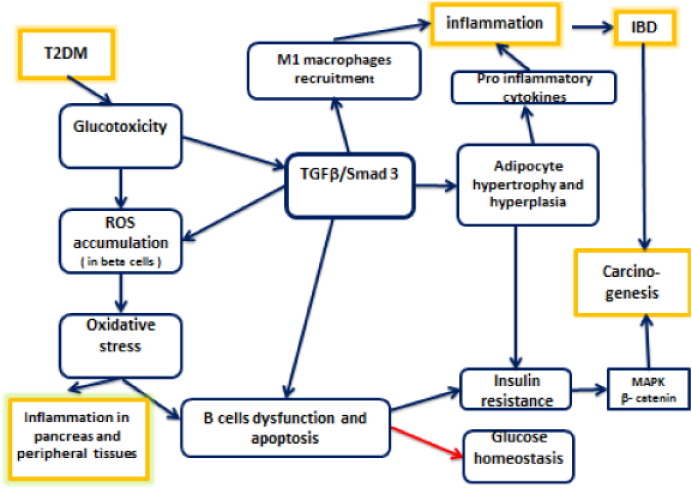
TGFβ plays a crucial role in pancreatic β cell malfunctioning as glucotoxicity stimulates its signaling cascade through smad 3, IL-6 and epithelial to mesenchymal transition. Such a cascade could lead to macrophages and other cells recruitment, inflammation, then IBD and CRC.
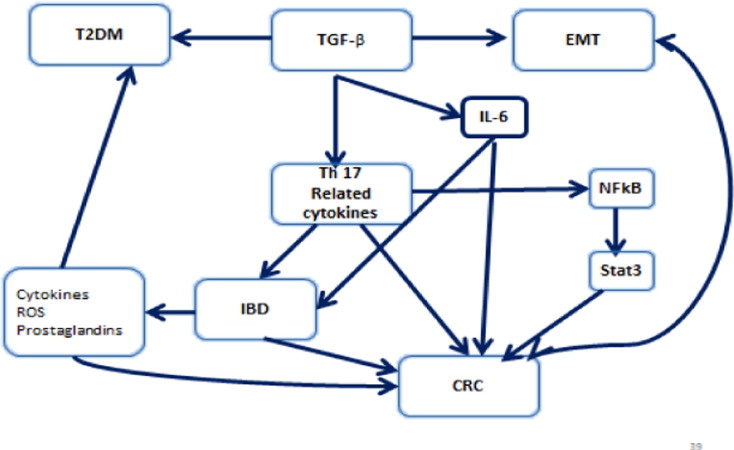
NFkB is also another key regulator in the crosstalk among the pathways leading to the three disease entities. It plays a major role in linking inflammation to cancer development through its ability to up regulate several inflammatory and tumor promoting cytokines like: IL-6, IL-1 α and TNF α, as well as genes like BCL2 and BCLXL. It activates JAK/STAT signaling network via STAT3 transcription factors and promotes epithelial to mesenchymal transition. It also increases the risk for T2DM in obese people. In brief, NFKB is a matchmaker between inflammation, IBD, cancer and diabetes.
In addition, TNFα plays a pivotal role in systemic inflammation. It is increased in the mucosa of IBD patients and has a central role in its pathogenesis. It also activates other signaling pathways like NFKB and MAPK leading to CRC. It is also overexpressed in the adipose tissues of obese patients thus linking it to T2DM, chronic inflammation and consequently CRC.
On the other hand, increasing evidence suggests that dysbiosis plays a role in initiating, maintaining and determining the severity of IBD. Actually, among its functions, it modulates genotoxic metabolites which are able to induce CRC, a fact proven to be sustained by stool transfer from patients with CRC. Probiotics, however, may actively prevent CRC as well as IBD and results in a significant decrease in fasting glycemia in T2DM patients.
In conclusion, IBD, CRC and T2DM are commonly occurring interrelated clinical problems. They share a common basis influenced by an inflammatory process, an imbalance in intestinal microbiota, and a crosstalk between various signaling pathways. Would probiotics interrupt the crosstalk or orient it in the physiological direction?

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


