{"title":"一种改进的图插管方法","authors":"William C. Bauer MS","doi":"10.1002/dat.20610","DOIUrl":null,"url":null,"abstract":"<p>The approach given here was studied on one patient (her third graft) with the following result. The graft endured for 6+ years of use (electively retired), which was three times longer than her two prior grafts, which were cannulated without this approach. Figure 1<i>A</i> and <i>B</i> are examples of the cannulation care plan for this patient, defined several years apart and edited for publication clarity (no substantive change).</p><p>For consistency, this author suggests that cannulation care contacts be assigned to define the cannulation care plans (Stage 1). It takes about 30 minutes per patient to complete Stage 1. The output is the cannulation care plan (as documented on the TF). Staff who can cannulate and “use a map” can implement the cannulation care plan (i.e., complete Stage 2), which takes about 5 minutes per patient per treatment. From time to time, an update to the cannulation care plan may also be needed during Stage 2. Nevertheless, the time differential to implement the cannulation care plan does not affect patient scheduling, since the lower frequency of minor complications (infiltration, oozing, pseudoaneurysm, pain) is likely to reduce time needed for the procedure, i.e., saving time via preventive action.</p><p>These additional medical costs are approximately $2,000 per incident.<span>2</span> More than 70,000 patients use grafts as their primary access.<span>3</span> If 2,500 access replacements are delayed per year by cannulation care plans (assumes 50 instances per state/year), then medical savings of $5,000,000/year ($2,000 × 2,500) are predicted with this approach.</p><p>Additional savings will apply if the frequency of thrombosis, stenoses, or infection is reduced by cannulation care plans. This topic merits study, as this patient's first and second (not the third) grafts incurred thrombectomies and infection. Angioplasty did not apply for this patient. Most important, extending longevity of grafts improves quality of life for patients.</p>","PeriodicalId":51012,"journal":{"name":"Dialysis & Transplantation","volume":"40 9","pages":"418-421"},"PeriodicalIF":0.0000,"publicationDate":"2011-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/dat.20610","citationCount":"0","resultStr":"{\"title\":\"An improved approach to graph cannulation\",\"authors\":\"William C. Bauer MS\",\"doi\":\"10.1002/dat.20610\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The approach given here was studied on one patient (her third graft) with the following result. The graft endured for 6+ years of use (electively retired), which was three times longer than her two prior grafts, which were cannulated without this approach. Figure 1<i>A</i> and <i>B</i> are examples of the cannulation care plan for this patient, defined several years apart and edited for publication clarity (no substantive change).</p><p>For consistency, this author suggests that cannulation care contacts be assigned to define the cannulation care plans (Stage 1). It takes about 30 minutes per patient to complete Stage 1. The output is the cannulation care plan (as documented on the TF). Staff who can cannulate and “use a map” can implement the cannulation care plan (i.e., complete Stage 2), which takes about 5 minutes per patient per treatment. From time to time, an update to the cannulation care plan may also be needed during Stage 2. Nevertheless, the time differential to implement the cannulation care plan does not affect patient scheduling, since the lower frequency of minor complications (infiltration, oozing, pseudoaneurysm, pain) is likely to reduce time needed for the procedure, i.e., saving time via preventive action.</p><p>These additional medical costs are approximately $2,000 per incident.<span>2</span> More than 70,000 patients use grafts as their primary access.<span>3</span> If 2,500 access replacements are delayed per year by cannulation care plans (assumes 50 instances per state/year), then medical savings of $5,000,000/year ($2,000 × 2,500) are predicted with this approach.</p><p>Additional savings will apply if the frequency of thrombosis, stenoses, or infection is reduced by cannulation care plans. This topic merits study, as this patient's first and second (not the third) grafts incurred thrombectomies and infection. Angioplasty did not apply for this patient. Most important, extending longevity of grafts improves quality of life for patients.</p>\",\"PeriodicalId\":51012,\"journal\":{\"name\":\"Dialysis & Transplantation\",\"volume\":\"40 9\",\"pages\":\"418-421\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-09-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/dat.20610\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Dialysis & Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/dat.20610\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dialysis & Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dat.20610","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
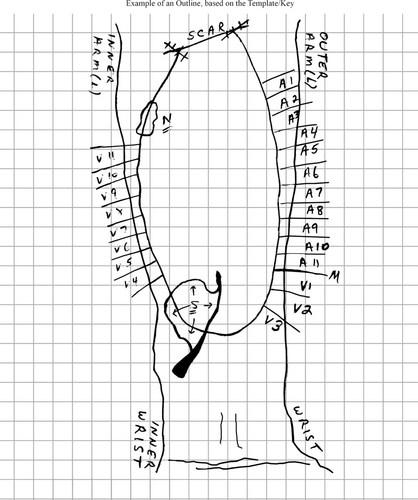
The approach given here was studied on one patient (her third graft) with the following result. The graft endured for 6+ years of use (electively retired), which was three times longer than her two prior grafts, which were cannulated without this approach. Figure 1A and B are examples of the cannulation care plan for this patient, defined several years apart and edited for publication clarity (no substantive change).
For consistency, this author suggests that cannulation care contacts be assigned to define the cannulation care plans (Stage 1). It takes about 30 minutes per patient to complete Stage 1. The output is the cannulation care plan (as documented on the TF). Staff who can cannulate and “use a map” can implement the cannulation care plan (i.e., complete Stage 2), which takes about 5 minutes per patient per treatment. From time to time, an update to the cannulation care plan may also be needed during Stage 2. Nevertheless, the time differential to implement the cannulation care plan does not affect patient scheduling, since the lower frequency of minor complications (infiltration, oozing, pseudoaneurysm, pain) is likely to reduce time needed for the procedure, i.e., saving time via preventive action.
These additional medical costs are approximately $2,000 per incident.2 More than 70,000 patients use grafts as their primary access.3 If 2,500 access replacements are delayed per year by cannulation care plans (assumes 50 instances per state/year), then medical savings of $5,000,000/year ($2,000 × 2,500) are predicted with this approach.
Additional savings will apply if the frequency of thrombosis, stenoses, or infection is reduced by cannulation care plans. This topic merits study, as this patient's first and second (not the third) grafts incurred thrombectomies and infection. Angioplasty did not apply for this patient. Most important, extending longevity of grafts improves quality of life for patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


