{"title":"NB-UVB联合德哥西替尼治疗顽固性湿疹患儿成功","authors":"Ichiro Kurokawa MD, Jun-Ichiro Ono MD","doi":"10.1002/cia2.12250","DOIUrl":null,"url":null,"abstract":"<p>A 4-year-old girl with refractory nummular eczema with atopic dermatitis (AD) was reported successfully treated with narrowband ultraviolet B (NB-UVB) once a week (400 mJ/cm<sup>2</sup>) and topical delgocitinib for 8 weeks. The treatment of NB-UVB and topical delgocitinib improved the severe nummular lesions and strong pruritus, resulting in only brown postinflammatory hyperpigmentation without pruritus. The combination of NB-UVB and topical delgocitinib can be an alternative treatment for refractory nummular eczema in children.</p><p>A 4-year-old girl presented with a 2-year history of AD. She had impetigo contagiosum throughout her body due to methicillin-resistant <i>Staphylococcus aureus</i> (MRSA) infection. Subsequently, nummular eczema with elevated erythema, erosion, and brown pigmentation occurred over the former impetigo lesions on the shoulders, buttocks (Figure 1A), and thighs with severe pruritus. She was treated with topical steroids, oral antihistamines, and antimicrobials. However, the patient did not respond to these treatments. Thus, NB-UVB therapy (400 mJ/cm<sup>2</sup>) once a week and topical delgocitinib twice a day were administered. After 8 weeks, the nummular eczema remarkably improved, resulting in flat brown pigmentation (Figure 1B). Laboratory findings showed eosinophilia (22%) and high immunoglobulin (Ig) E levels (853 IU/ml). Radioallergosorbent test (RAST) had a score of 6 (House dust 1 and dust mite). Bacterial culture from nummular eczema was negative.</p><p>Topical corticosteroids, antihistamines, and antimicrobials were ineffective in our case. NB-UVB therapy is a tolerant and effective treatment for children with AD.<span><sup>1</sup></span> NB-UVB inhibits immunological reactions and has anti-inflammatory and anti-bacterial effects. It also recovers skin barrier defects.<span><sup>2</sup></span> Therefore, NB-UVB therapy is a tolerant and economical treatment for children with AD. Moreover, it inhibits immune reactions, cytotoxic effects, cis-urocanic induction, and decreases Langerhans cells, antigen presentation, NK cell activity, and apoptosis of T cells and keratinocytes.<span><sup>3</sup></span> However, the side effects of NB-UVB include erythema, reactivation of herpes simplex, and polymorphous light eruption.</p><p>Delgocitinib, a Janus kinase (JAK) inhibitor, is useful for treating AD.<span><sup>4</sup></span> It is available for children with AD with ages more than 2 years old.<span><sup>5</sup></span> It inhibits IL-4, IL-13, and IL-31,<span><sup>6</sup></span> resulting in the relief of pruritus.</p><p>In our case, the patient did not respond to topical corticosteroids, antihistamines, or oral antimicrobials. We preferred NB-UVB and topical delgocitinib treatments. We speculated that the synergistic effects of NB-UVB and delgocitinib improved the refractory nummular eczema.</p><p>In our case, to reduce the risk, we should have tried to use topical delgocitinib alone at first. Additionally, the safety of long-term NB treatment for children has not been established. Therefore, targeted phototherapy was more preferable to use for children to minimize the risk. Moreover, the safety of the combination of NB and topical delgocitinib has not been established in safety for the risk of skin tumor.<span><sup>7</sup></span> Therefore, the careful observation in our case should be necessary in the future.</p><p>In conclusion, NB-UVB and topical delgocitinib are possible alternative treatments for refractory nummular eczema in children. Further studies on such cases must be accumulated in the future.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A</p><p>Informed Consent: Written informed consent was obtained from the patient's mother.</p><p>Registry and the Registration No. of the study/trial: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"5 6","pages":"229-230"},"PeriodicalIF":0.9000,"publicationDate":"2022-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12250","citationCount":"1","resultStr":"{\"title\":\"Refractory nummular eczema in child successfully treated with NB-UVB and topical delgocitinib\",\"authors\":\"Ichiro Kurokawa MD, Jun-Ichiro Ono MD\",\"doi\":\"10.1002/cia2.12250\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 4-year-old girl with refractory nummular eczema with atopic dermatitis (AD) was reported successfully treated with narrowband ultraviolet B (NB-UVB) once a week (400 mJ/cm<sup>2</sup>) and topical delgocitinib for 8 weeks. The treatment of NB-UVB and topical delgocitinib improved the severe nummular lesions and strong pruritus, resulting in only brown postinflammatory hyperpigmentation without pruritus. The combination of NB-UVB and topical delgocitinib can be an alternative treatment for refractory nummular eczema in children.</p><p>A 4-year-old girl presented with a 2-year history of AD. She had impetigo contagiosum throughout her body due to methicillin-resistant <i>Staphylococcus aureus</i> (MRSA) infection. Subsequently, nummular eczema with elevated erythema, erosion, and brown pigmentation occurred over the former impetigo lesions on the shoulders, buttocks (Figure 1A), and thighs with severe pruritus. She was treated with topical steroids, oral antihistamines, and antimicrobials. However, the patient did not respond to these treatments. Thus, NB-UVB therapy (400 mJ/cm<sup>2</sup>) once a week and topical delgocitinib twice a day were administered. After 8 weeks, the nummular eczema remarkably improved, resulting in flat brown pigmentation (Figure 1B). Laboratory findings showed eosinophilia (22%) and high immunoglobulin (Ig) E levels (853 IU/ml). Radioallergosorbent test (RAST) had a score of 6 (House dust 1 and dust mite). Bacterial culture from nummular eczema was negative.</p><p>Topical corticosteroids, antihistamines, and antimicrobials were ineffective in our case. NB-UVB therapy is a tolerant and effective treatment for children with AD.<span><sup>1</sup></span> NB-UVB inhibits immunological reactions and has anti-inflammatory and anti-bacterial effects. It also recovers skin barrier defects.<span><sup>2</sup></span> Therefore, NB-UVB therapy is a tolerant and economical treatment for children with AD. Moreover, it inhibits immune reactions, cytotoxic effects, cis-urocanic induction, and decreases Langerhans cells, antigen presentation, NK cell activity, and apoptosis of T cells and keratinocytes.<span><sup>3</sup></span> However, the side effects of NB-UVB include erythema, reactivation of herpes simplex, and polymorphous light eruption.</p><p>Delgocitinib, a Janus kinase (JAK) inhibitor, is useful for treating AD.<span><sup>4</sup></span> It is available for children with AD with ages more than 2 years old.<span><sup>5</sup></span> It inhibits IL-4, IL-13, and IL-31,<span><sup>6</sup></span> resulting in the relief of pruritus.</p><p>In our case, the patient did not respond to topical corticosteroids, antihistamines, or oral antimicrobials. We preferred NB-UVB and topical delgocitinib treatments. We speculated that the synergistic effects of NB-UVB and delgocitinib improved the refractory nummular eczema.</p><p>In our case, to reduce the risk, we should have tried to use topical delgocitinib alone at first. Additionally, the safety of long-term NB treatment for children has not been established. Therefore, targeted phototherapy was more preferable to use for children to minimize the risk. Moreover, the safety of the combination of NB and topical delgocitinib has not been established in safety for the risk of skin tumor.<span><sup>7</sup></span> Therefore, the careful observation in our case should be necessary in the future.</p><p>In conclusion, NB-UVB and topical delgocitinib are possible alternative treatments for refractory nummular eczema in children. Further studies on such cases must be accumulated in the future.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A</p><p>Informed Consent: Written informed consent was obtained from the patient's mother.</p><p>Registry and the Registration No. of the study/trial: N/A.</p><p>Animal Studies: N/A.</p>\",\"PeriodicalId\":15543,\"journal\":{\"name\":\"Journal of Cutaneous Immunology and Allergy\",\"volume\":\"5 6\",\"pages\":\"229-230\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2022-05-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12250\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cutaneous Immunology and Allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12250\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
Refractory nummular eczema in child successfully treated with NB-UVB and topical delgocitinib
A 4-year-old girl with refractory nummular eczema with atopic dermatitis (AD) was reported successfully treated with narrowband ultraviolet B (NB-UVB) once a week (400 mJ/cm2) and topical delgocitinib for 8 weeks. The treatment of NB-UVB and topical delgocitinib improved the severe nummular lesions and strong pruritus, resulting in only brown postinflammatory hyperpigmentation without pruritus. The combination of NB-UVB and topical delgocitinib can be an alternative treatment for refractory nummular eczema in children.
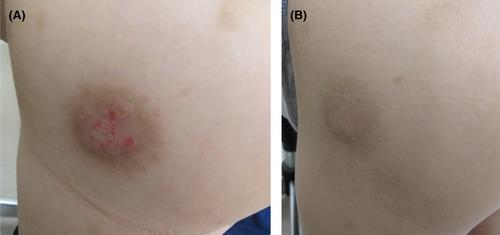
A 4-year-old girl presented with a 2-year history of AD. She had impetigo contagiosum throughout her body due to methicillin-resistant Staphylococcus aureus (MRSA) infection. Subsequently, nummular eczema with elevated erythema, erosion, and brown pigmentation occurred over the former impetigo lesions on the shoulders, buttocks (Figure 1A), and thighs with severe pruritus. She was treated with topical steroids, oral antihistamines, and antimicrobials. However, the patient did not respond to these treatments. Thus, NB-UVB therapy (400 mJ/cm2) once a week and topical delgocitinib twice a day were administered. After 8 weeks, the nummular eczema remarkably improved, resulting in flat brown pigmentation (Figure 1B). Laboratory findings showed eosinophilia (22%) and high immunoglobulin (Ig) E levels (853 IU/ml). Radioallergosorbent test (RAST) had a score of 6 (House dust 1 and dust mite). Bacterial culture from nummular eczema was negative.
Topical corticosteroids, antihistamines, and antimicrobials were ineffective in our case. NB-UVB therapy is a tolerant and effective treatment for children with AD.1 NB-UVB inhibits immunological reactions and has anti-inflammatory and anti-bacterial effects. It also recovers skin barrier defects.2 Therefore, NB-UVB therapy is a tolerant and economical treatment for children with AD. Moreover, it inhibits immune reactions, cytotoxic effects, cis-urocanic induction, and decreases Langerhans cells, antigen presentation, NK cell activity, and apoptosis of T cells and keratinocytes.3 However, the side effects of NB-UVB include erythema, reactivation of herpes simplex, and polymorphous light eruption.
Delgocitinib, a Janus kinase (JAK) inhibitor, is useful for treating AD.4 It is available for children with AD with ages more than 2 years old.5 It inhibits IL-4, IL-13, and IL-31,6 resulting in the relief of pruritus.
In our case, the patient did not respond to topical corticosteroids, antihistamines, or oral antimicrobials. We preferred NB-UVB and topical delgocitinib treatments. We speculated that the synergistic effects of NB-UVB and delgocitinib improved the refractory nummular eczema.
In our case, to reduce the risk, we should have tried to use topical delgocitinib alone at first. Additionally, the safety of long-term NB treatment for children has not been established. Therefore, targeted phototherapy was more preferable to use for children to minimize the risk. Moreover, the safety of the combination of NB and topical delgocitinib has not been established in safety for the risk of skin tumor.7 Therefore, the careful observation in our case should be necessary in the future.
In conclusion, NB-UVB and topical delgocitinib are possible alternative treatments for refractory nummular eczema in children. Further studies on such cases must be accumulated in the future.
The authors declare no conflict of interest.
Approval of the research protocol: N/A
Informed Consent: Written informed consent was obtained from the patient's mother.
Registry and the Registration No. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


