{"title":"免疫检查点抑制剂介导的肝毒性的发生率和治疗策略:系统综述","authors":"Kang Miao, Li Zhang","doi":"10.1016/j.cpt.2022.11.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>A hepatic adverse event (HAE) is defined as a liver injury that occurs following immune checkpoint inhibitor (ICI) administration in oncology Patients. Immune-mediated hepatotoxicity (IMH) is a type of HAE directly caused by ICI and is associated with immune system hyperactivation. HAE incidence varies across different clinical studies. This study aimed to explore the risk factors of HAE and establish a personalized IMH treatment strategy.</p></div><div><h3>Methods</h3><p>Randomized controlled trials (RCTs) on ICIs and case reports related to IMH were collected and summarized separately. Meta-analysis was performed using Review Manager (version 5.0), whereas correlation analysis and linear regression were performed using SPSS (version 24.0) to evaluate any correlations between the two variables.</p></div><div><h3>Results</h3><p>Overall, 36 RCTs containing 18,515 patients and 39 case reports met our inclusion criteria. The ICI administration increased the HAE risk (risk ratio [RR] = 1.40) as well as severe HAE (RR = 2.55). The overall HAE incidence and severe incidence were about 15.3% and 4.3%, respectively. Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors have a higher incidence of HAE than programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1) inhibitors. Finally, we found a positive correlation between the onset time of IMH and the recovery time of liver injury.</p></div><div><h3>Conclusions</h3><p>ICI administration increased the incidence risk of HAE, especially in patients treated with CTLA-4 inhibitors. Regarding IMH treatment, the glucocorticoid dosage must be individually reduced according to the severity and onset time of HAE.</p></div>","PeriodicalId":93920,"journal":{"name":"Cancer pathogenesis and therapy","volume":"1 1","pages":"Pages 46-55"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Incidence rate and treatment strategy of immune checkpoint inhibitor mediated hepatotoxicity: A systematic review\",\"authors\":\"Kang Miao, Li Zhang\",\"doi\":\"10.1016/j.cpt.2022.11.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>A hepatic adverse event (HAE) is defined as a liver injury that occurs following immune checkpoint inhibitor (ICI) administration in oncology Patients. Immune-mediated hepatotoxicity (IMH) is a type of HAE directly caused by ICI and is associated with immune system hyperactivation. HAE incidence varies across different clinical studies. This study aimed to explore the risk factors of HAE and establish a personalized IMH treatment strategy.</p></div><div><h3>Methods</h3><p>Randomized controlled trials (RCTs) on ICIs and case reports related to IMH were collected and summarized separately. Meta-analysis was performed using Review Manager (version 5.0), whereas correlation analysis and linear regression were performed using SPSS (version 24.0) to evaluate any correlations between the two variables.</p></div><div><h3>Results</h3><p>Overall, 36 RCTs containing 18,515 patients and 39 case reports met our inclusion criteria. The ICI administration increased the HAE risk (risk ratio [RR] = 1.40) as well as severe HAE (RR = 2.55). The overall HAE incidence and severe incidence were about 15.3% and 4.3%, respectively. Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors have a higher incidence of HAE than programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1) inhibitors. Finally, we found a positive correlation between the onset time of IMH and the recovery time of liver injury.</p></div><div><h3>Conclusions</h3><p>ICI administration increased the incidence risk of HAE, especially in patients treated with CTLA-4 inhibitors. Regarding IMH treatment, the glucocorticoid dosage must be individually reduced according to the severity and onset time of HAE.</p></div>\",\"PeriodicalId\":93920,\"journal\":{\"name\":\"Cancer pathogenesis and therapy\",\"volume\":\"1 1\",\"pages\":\"Pages 46-55\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer pathogenesis and therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S294971322200012X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer pathogenesis and therapy","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S294971322200012X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Incidence rate and treatment strategy of immune checkpoint inhibitor mediated hepatotoxicity: A systematic review
Background
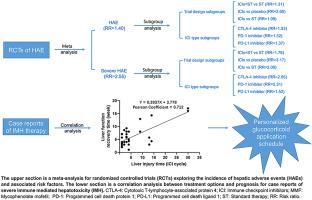
A hepatic adverse event (HAE) is defined as a liver injury that occurs following immune checkpoint inhibitor (ICI) administration in oncology Patients. Immune-mediated hepatotoxicity (IMH) is a type of HAE directly caused by ICI and is associated with immune system hyperactivation. HAE incidence varies across different clinical studies. This study aimed to explore the risk factors of HAE and establish a personalized IMH treatment strategy.
Methods
Randomized controlled trials (RCTs) on ICIs and case reports related to IMH were collected and summarized separately. Meta-analysis was performed using Review Manager (version 5.0), whereas correlation analysis and linear regression were performed using SPSS (version 24.0) to evaluate any correlations between the two variables.
Results
Overall, 36 RCTs containing 18,515 patients and 39 case reports met our inclusion criteria. The ICI administration increased the HAE risk (risk ratio [RR] = 1.40) as well as severe HAE (RR = 2.55). The overall HAE incidence and severe incidence were about 15.3% and 4.3%, respectively. Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors have a higher incidence of HAE than programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1) inhibitors. Finally, we found a positive correlation between the onset time of IMH and the recovery time of liver injury.
Conclusions
ICI administration increased the incidence risk of HAE, especially in patients treated with CTLA-4 inhibitors. Regarding IMH treatment, the glucocorticoid dosage must be individually reduced according to the severity and onset time of HAE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


