Emily P. Zeitler MD, MHS, Joanna Joly MD, Christopher G. Leggett PhD, Sandra L. Wong MD, MS, A. James O'Malley PhD, Sally A. Kraft MD, MPH, Matthew B. Mackwood MD, MPH, Sarah T. Jones MPH, Jonathan S. Skinner PhD
{"title":"合并症、药物和健康的社会决定因素在理解心力衰竭患者城乡结局差异中的作用。","authors":"Emily P. Zeitler MD, MHS, Joanna Joly MD, Christopher G. Leggett PhD, Sandra L. Wong MD, MS, A. James O'Malley PhD, Sally A. Kraft MD, MPH, Matthew B. Mackwood MD, MPH, Sarah T. Jones MPH, Jonathan S. Skinner PhD","doi":"10.1111/jrh.12803","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Purpose</h3>\n \n <p>There is now a 20% disparity in all-cause, excess deaths between urban and rural areas, much of which is driven by disparities in cardiovascular death. We sought to explain the sources of these disparities for Medicare beneficiaries with heart failure with reduced ejection fraction (HFrEF).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Using a sample of Medicare Parts A, B, and D, we created a cohort of 389,528 fee-for-service beneficiaries with at least 1 heart failure hospitalization from 2008 to 2017. The primary outcome was 30-day mortality after discharge; 1-year mortality, readmissions, and return emergency room (ER) admissions were secondary outcomes. We used hierarchical, logistic regression modeling to determine the contribution of comorbidities, guideline-directed medical therapy (GDMT), and social determinants of health (SDOH) to outcomes.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Thirty-day mortality rates after hospital discharge were 6.3% in rural areas compared to 5.7% in urban regions (<i>P</i> < .001); after adjusting for patient health and GDMT receipt, the 30-day mortality odds ratio for rural residence was 1.201 (95% CI 1.164-1.239). Adding the SDOH measure reduced the odds ratio somewhat (1.140, 95% CI 1.103-1.178) but a gap remained. Readmission rates in rural areas were consistently lower for all model specifications, while ER admissions were consistently higher.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Among patients with HFrEF, living in a rural area is associated with an increased risk of death and return ER visits within 30 days of discharge from HF hospitalization. Differences in SDOH appear to partially explain mortality differences but the remaining gap may be the consequence of rural-urban differences in HF treatment.</p>\n </section>\n </div>","PeriodicalId":50060,"journal":{"name":"Journal of Rural Health","volume":"40 2","pages":"386-393"},"PeriodicalIF":2.7000,"publicationDate":"2023-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jrh.12803","citationCount":"0","resultStr":"{\"title\":\"The role of comorbidities, medications, and social determinants of health in understanding urban-rural outcome differences among patients with heart failure\",\"authors\":\"Emily P. Zeitler MD, MHS, Joanna Joly MD, Christopher G. Leggett PhD, Sandra L. Wong MD, MS, A. James O'Malley PhD, Sally A. Kraft MD, MPH, Matthew B. Mackwood MD, MPH, Sarah T. Jones MPH, Jonathan S. Skinner PhD\",\"doi\":\"10.1111/jrh.12803\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Purpose</h3>\\n \\n <p>There is now a 20% disparity in all-cause, excess deaths between urban and rural areas, much of which is driven by disparities in cardiovascular death. We sought to explain the sources of these disparities for Medicare beneficiaries with heart failure with reduced ejection fraction (HFrEF).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Using a sample of Medicare Parts A, B, and D, we created a cohort of 389,528 fee-for-service beneficiaries with at least 1 heart failure hospitalization from 2008 to 2017. The primary outcome was 30-day mortality after discharge; 1-year mortality, readmissions, and return emergency room (ER) admissions were secondary outcomes. We used hierarchical, logistic regression modeling to determine the contribution of comorbidities, guideline-directed medical therapy (GDMT), and social determinants of health (SDOH) to outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Thirty-day mortality rates after hospital discharge were 6.3% in rural areas compared to 5.7% in urban regions (<i>P</i> < .001); after adjusting for patient health and GDMT receipt, the 30-day mortality odds ratio for rural residence was 1.201 (95% CI 1.164-1.239). Adding the SDOH measure reduced the odds ratio somewhat (1.140, 95% CI 1.103-1.178) but a gap remained. Readmission rates in rural areas were consistently lower for all model specifications, while ER admissions were consistently higher.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Among patients with HFrEF, living in a rural area is associated with an increased risk of death and return ER visits within 30 days of discharge from HF hospitalization. Differences in SDOH appear to partially explain mortality differences but the remaining gap may be the consequence of rural-urban differences in HF treatment.</p>\\n </section>\\n </div>\",\"PeriodicalId\":50060,\"journal\":{\"name\":\"Journal of Rural Health\",\"volume\":\"40 2\",\"pages\":\"386-393\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2023-10-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jrh.12803\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Rural Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jrh.12803\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Rural Health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jrh.12803","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
The role of comorbidities, medications, and social determinants of health in understanding urban-rural outcome differences among patients with heart failure
Purpose
There is now a 20% disparity in all-cause, excess deaths between urban and rural areas, much of which is driven by disparities in cardiovascular death. We sought to explain the sources of these disparities for Medicare beneficiaries with heart failure with reduced ejection fraction (HFrEF).
Methods
Using a sample of Medicare Parts A, B, and D, we created a cohort of 389,528 fee-for-service beneficiaries with at least 1 heart failure hospitalization from 2008 to 2017. The primary outcome was 30-day mortality after discharge; 1-year mortality, readmissions, and return emergency room (ER) admissions were secondary outcomes. We used hierarchical, logistic regression modeling to determine the contribution of comorbidities, guideline-directed medical therapy (GDMT), and social determinants of health (SDOH) to outcomes.
Results
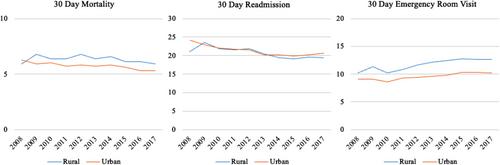
Thirty-day mortality rates after hospital discharge were 6.3% in rural areas compared to 5.7% in urban regions (P < .001); after adjusting for patient health and GDMT receipt, the 30-day mortality odds ratio for rural residence was 1.201 (95% CI 1.164-1.239). Adding the SDOH measure reduced the odds ratio somewhat (1.140, 95% CI 1.103-1.178) but a gap remained. Readmission rates in rural areas were consistently lower for all model specifications, while ER admissions were consistently higher.
Conclusions
Among patients with HFrEF, living in a rural area is associated with an increased risk of death and return ER visits within 30 days of discharge from HF hospitalization. Differences in SDOH appear to partially explain mortality differences but the remaining gap may be the consequence of rural-urban differences in HF treatment.
期刊介绍:
The Journal of Rural Health, a quarterly journal published by the NRHA, offers a variety of original research relevant and important to rural health. Some examples include evaluations, case studies, and analyses related to health status and behavior, as well as to health work force, policy and access issues. Quantitative, qualitative and mixed methods studies are welcome. Highest priority is given to manuscripts that reflect scholarly quality, demonstrate methodological rigor, and emphasize practical implications. The journal also publishes articles with an international rural health perspective, commentaries, book reviews and letters.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


