{"title":"探查性剖腹探查术后早期造口旁切除术:一例罕见且可能危及生命的手术并发症的病例报告。","authors":"Anis Hasnaoui, Racem Trigui, Sihem Heni, Salma Kacem","doi":"10.1186/s13037-023-00379-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Parastomal evisceration represents a preventable surgical complication that should not occur with appropriate technical diligence and surgical skills. While late parastomal hernias are well described in the literature, there is a paucity of reports on the early postoperative occurrence of parastomal intestinal evisceration.</p><p><strong>Case presentation: </strong>An urgent laparotomy was performed on a 58-year-old female patient for an acute cecal perforation with generalized peritonitis related to underlying colon cancer. Intraoperative revelations necessitated a carcinologic right colectomy and the creation of an end-loop ileocolostomy. Following six sessions of adjuvant chemotherapy, Computed tomography scans raised uncertainties about the presence of peritoneal carcinomatosis. Consequently, a collaborative decision was reached in a multidisciplinary discussion to conduct a surgical biopsy of these deposits before reinstating digestive continuity. The surgical procedure started with stoma mobilization. However, adhesions and a relatively confined aperture curtailed a comprehensive peritoneal cavity exploration. Thus, a midline incision was executed. The verdict from the frozen section examination affirmed metastatic presence, prompting the retention of the stoma. Within 48 h post-surgery, an early-stage parastomal evisceration occurred, stemming from an inadequately sealed aponeurotic sheath. The exposed bowel surface was encased in fibrin, necessitating meticulous irrigation with a warm saline solution before repositioning it within the peritoneal cavity. Accurate adjustment of the aponeurosis closure ensued, coupled with a meticulous reconstitution of the stoma. The postoperative course was uneventful. The patient was subsequently referred for hyperthermic intraperitoneal chemotherapy.</p><p><strong>Conclusions: </strong>Preventing parastomal evisceration requires adherence to established stoma-creation protocols, including creating a properly sized fascial opening and secure fixation. In instances of excessive fascial opening, ensuring a tension-free and meticulous closure is imperative.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"17 1","pages":"26"},"PeriodicalIF":2.6000,"publicationDate":"2023-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10591356/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early postoperative parastomal evisceration after explorative laparotomy: case report of a rare and potentially life-threatening surgical complication.\",\"authors\":\"Anis Hasnaoui, Racem Trigui, Sihem Heni, Salma Kacem\",\"doi\":\"10.1186/s13037-023-00379-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Parastomal evisceration represents a preventable surgical complication that should not occur with appropriate technical diligence and surgical skills. While late parastomal hernias are well described in the literature, there is a paucity of reports on the early postoperative occurrence of parastomal intestinal evisceration.</p><p><strong>Case presentation: </strong>An urgent laparotomy was performed on a 58-year-old female patient for an acute cecal perforation with generalized peritonitis related to underlying colon cancer. Intraoperative revelations necessitated a carcinologic right colectomy and the creation of an end-loop ileocolostomy. Following six sessions of adjuvant chemotherapy, Computed tomography scans raised uncertainties about the presence of peritoneal carcinomatosis. Consequently, a collaborative decision was reached in a multidisciplinary discussion to conduct a surgical biopsy of these deposits before reinstating digestive continuity. The surgical procedure started with stoma mobilization. However, adhesions and a relatively confined aperture curtailed a comprehensive peritoneal cavity exploration. Thus, a midline incision was executed. The verdict from the frozen section examination affirmed metastatic presence, prompting the retention of the stoma. Within 48 h post-surgery, an early-stage parastomal evisceration occurred, stemming from an inadequately sealed aponeurotic sheath. The exposed bowel surface was encased in fibrin, necessitating meticulous irrigation with a warm saline solution before repositioning it within the peritoneal cavity. Accurate adjustment of the aponeurosis closure ensued, coupled with a meticulous reconstitution of the stoma. The postoperative course was uneventful. The patient was subsequently referred for hyperthermic intraperitoneal chemotherapy.</p><p><strong>Conclusions: </strong>Preventing parastomal evisceration requires adherence to established stoma-creation protocols, including creating a properly sized fascial opening and secure fixation. In instances of excessive fascial opening, ensuring a tension-free and meticulous closure is imperative.</p>\",\"PeriodicalId\":46782,\"journal\":{\"name\":\"Patient Safety in Surgery\",\"volume\":\"17 1\",\"pages\":\"26\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-10-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10591356/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Patient Safety in Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13037-023-00379-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-023-00379-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Early postoperative parastomal evisceration after explorative laparotomy: case report of a rare and potentially life-threatening surgical complication.
Background: Parastomal evisceration represents a preventable surgical complication that should not occur with appropriate technical diligence and surgical skills. While late parastomal hernias are well described in the literature, there is a paucity of reports on the early postoperative occurrence of parastomal intestinal evisceration.
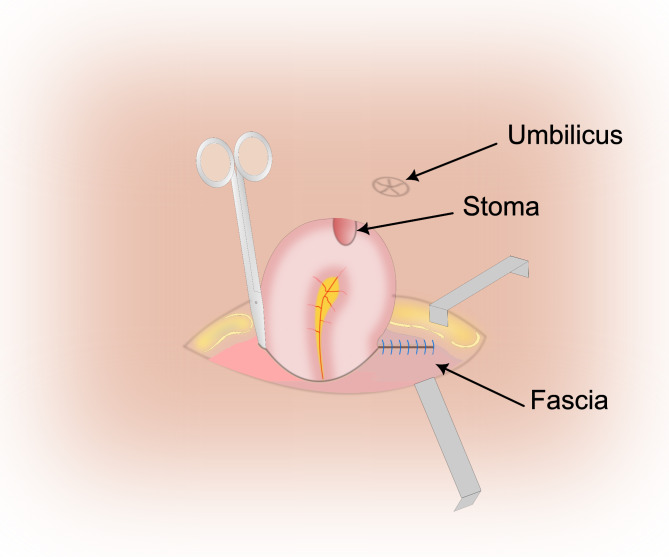
Case presentation: An urgent laparotomy was performed on a 58-year-old female patient for an acute cecal perforation with generalized peritonitis related to underlying colon cancer. Intraoperative revelations necessitated a carcinologic right colectomy and the creation of an end-loop ileocolostomy. Following six sessions of adjuvant chemotherapy, Computed tomography scans raised uncertainties about the presence of peritoneal carcinomatosis. Consequently, a collaborative decision was reached in a multidisciplinary discussion to conduct a surgical biopsy of these deposits before reinstating digestive continuity. The surgical procedure started with stoma mobilization. However, adhesions and a relatively confined aperture curtailed a comprehensive peritoneal cavity exploration. Thus, a midline incision was executed. The verdict from the frozen section examination affirmed metastatic presence, prompting the retention of the stoma. Within 48 h post-surgery, an early-stage parastomal evisceration occurred, stemming from an inadequately sealed aponeurotic sheath. The exposed bowel surface was encased in fibrin, necessitating meticulous irrigation with a warm saline solution before repositioning it within the peritoneal cavity. Accurate adjustment of the aponeurosis closure ensued, coupled with a meticulous reconstitution of the stoma. The postoperative course was uneventful. The patient was subsequently referred for hyperthermic intraperitoneal chemotherapy.
Conclusions: Preventing parastomal evisceration requires adherence to established stoma-creation protocols, including creating a properly sized fascial opening and secure fixation. In instances of excessive fascial opening, ensuring a tension-free and meticulous closure is imperative.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


