Ronda F Greaves, Monish Kumar, Nazha Mawad, Alberto Francescon, Chris Le, Michele O'Connell, James Chi, James Pitt
{"title":"鉴定经典21-羟化酶缺乏症的最佳实践应包括21-脱氧皮质醇分析和适当的异构体类固醇分离。","authors":"Ronda F Greaves, Monish Kumar, Nazha Mawad, Alberto Francescon, Chris Le, Michele O'Connell, James Chi, James Pitt","doi":"10.3390/ijns9040058","DOIUrl":null,"url":null,"abstract":"<p><p>There are mixed reports on the inclusion and use of 21 deoxycortisol (21DF) as the primary decision marker for classical 21-hydroxylase deficiency. We hypothesize that this may be due to insufficient recognition of the presence and chromatographic separation of isomeric steroids. The aim of this study was to determine the comparative utility of 21DF for screening and diagnosis of CAH due to classical 21-hydroxylase deficiency using a second-tier LC-MS/MS method that included the separation of isomeric steroids to 17OHP and 21DF. For each baby sample, one 3.2 mm dried blood spot was eluted in a methanolic solution containing isotopically matched internal standards. Data were interrogated by univariate and receiver operator characteristic analysis. Steroid profile results were generated for 924 non-CAH baby samples (median gestational age 37 weeks, range 22 to 43 weeks) and 17 babies with 21-hydroxylase deficiency. The ROC curves demonstrated 21DF to have the best sensitivity and specificity for the diagnosis of classical 21-hydroxylase deficiency with an AUC = 1.0. The heatmap showed the very strong correlation (r = 0.83) between 17OHP and 21DF. Our data support 21DF as a robust marker for CAH due to 21-hydroxylase deficiency. We recommend that 21DF be incorporated into routine newborn screening panels as part of the second-tier LC-MS/MS method, follow-up plasma steroid panels, and external quality assurance material.</p>","PeriodicalId":14159,"journal":{"name":"International Journal of Neonatal Screening","volume":"9 4","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2023-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594498/pdf/","citationCount":"0","resultStr":"{\"title\":\"Best Practice for Identification of Classical 21-Hydroxylase Deficiency Should Include 21 Deoxycortisol Analysis with Appropriate Isomeric Steroid Separation.\",\"authors\":\"Ronda F Greaves, Monish Kumar, Nazha Mawad, Alberto Francescon, Chris Le, Michele O'Connell, James Chi, James Pitt\",\"doi\":\"10.3390/ijns9040058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>There are mixed reports on the inclusion and use of 21 deoxycortisol (21DF) as the primary decision marker for classical 21-hydroxylase deficiency. We hypothesize that this may be due to insufficient recognition of the presence and chromatographic separation of isomeric steroids. The aim of this study was to determine the comparative utility of 21DF for screening and diagnosis of CAH due to classical 21-hydroxylase deficiency using a second-tier LC-MS/MS method that included the separation of isomeric steroids to 17OHP and 21DF. For each baby sample, one 3.2 mm dried blood spot was eluted in a methanolic solution containing isotopically matched internal standards. Data were interrogated by univariate and receiver operator characteristic analysis. Steroid profile results were generated for 924 non-CAH baby samples (median gestational age 37 weeks, range 22 to 43 weeks) and 17 babies with 21-hydroxylase deficiency. The ROC curves demonstrated 21DF to have the best sensitivity and specificity for the diagnosis of classical 21-hydroxylase deficiency with an AUC = 1.0. The heatmap showed the very strong correlation (r = 0.83) between 17OHP and 21DF. Our data support 21DF as a robust marker for CAH due to 21-hydroxylase deficiency. We recommend that 21DF be incorporated into routine newborn screening panels as part of the second-tier LC-MS/MS method, follow-up plasma steroid panels, and external quality assurance material.</p>\",\"PeriodicalId\":14159,\"journal\":{\"name\":\"International Journal of Neonatal Screening\",\"volume\":\"9 4\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-10-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594498/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Neonatal Screening\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/ijns9040058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GENETICS & HEREDITY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Neonatal Screening","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/ijns9040058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
Best Practice for Identification of Classical 21-Hydroxylase Deficiency Should Include 21 Deoxycortisol Analysis with Appropriate Isomeric Steroid Separation.
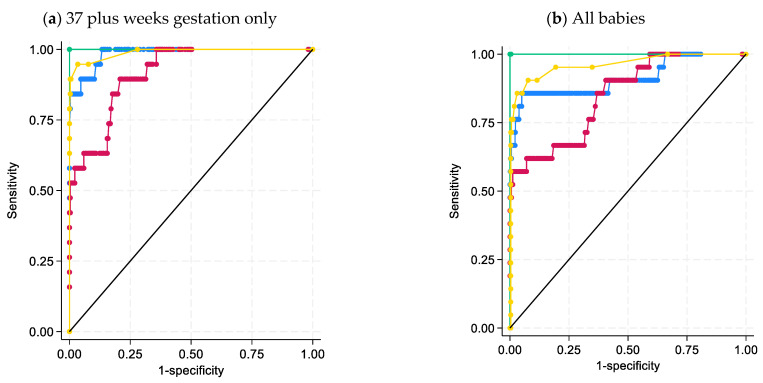
There are mixed reports on the inclusion and use of 21 deoxycortisol (21DF) as the primary decision marker for classical 21-hydroxylase deficiency. We hypothesize that this may be due to insufficient recognition of the presence and chromatographic separation of isomeric steroids. The aim of this study was to determine the comparative utility of 21DF for screening and diagnosis of CAH due to classical 21-hydroxylase deficiency using a second-tier LC-MS/MS method that included the separation of isomeric steroids to 17OHP and 21DF. For each baby sample, one 3.2 mm dried blood spot was eluted in a methanolic solution containing isotopically matched internal standards. Data were interrogated by univariate and receiver operator characteristic analysis. Steroid profile results were generated for 924 non-CAH baby samples (median gestational age 37 weeks, range 22 to 43 weeks) and 17 babies with 21-hydroxylase deficiency. The ROC curves demonstrated 21DF to have the best sensitivity and specificity for the diagnosis of classical 21-hydroxylase deficiency with an AUC = 1.0. The heatmap showed the very strong correlation (r = 0.83) between 17OHP and 21DF. Our data support 21DF as a robust marker for CAH due to 21-hydroxylase deficiency. We recommend that 21DF be incorporated into routine newborn screening panels as part of the second-tier LC-MS/MS method, follow-up plasma steroid panels, and external quality assurance material.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


