Nkechi Arinze, Nivin Omar, Amany Keruakous, Ravindra Kolhe, Natasha Savage
{"title":"推动考虑成人白血病/具有芽细胞形态的淋巴瘤的套细胞淋巴瘤。","authors":"Nkechi Arinze, Nivin Omar, Amany Keruakous, Ravindra Kolhe, Natasha Savage","doi":"10.3390/hematolrep15040061","DOIUrl":null,"url":null,"abstract":"<p><p>Mantle cell lymphoma (MCL) is an intermediate-grade B-cell lymphoma, representing 2.8% of all non-Hodgkin lymphomas in the US. It is associated with t(11;14)(q13; q23), which leads to the overexpression of cyclin D1, consequently promoting cell proliferation. MCL usually expresses CD19, CD20, CD43, surface immunoglobulins, FMC7, BCL2, cyclin D1, CD5, and SOX11. Herein is a case of a 67-year-old male, referred to our facility with shortness of breath, anemia (hemoglobin of 5.3 g/dL), thrombocytopenia (12 × 10<sup>9</sup>/L), and leukocytosis (283 × 10<sup>9</sup>/L). A peripheral blood smear showed marked lymphocytosis with blastoid morphology. Morphologic examination of the bone marrow biopsy revealed a diffuse sheet of blastoid cells expressing CD20 and CD10, but without CD5 or cyclin D1. Given these features, a differential diagnosis of diffuse large B-cell lymphoma (DLBCL) with germinal center derivation, high-grade follicular lymphoma, and Burkitt lymphoma was considered, with the latter not favored due to morphology. Additional studies revealed positive SOX11, and fluorescence in situ hybridization (FISH) studies detected t(11;14). These additional studies supported diagnosis of the blastoid variant of MCL. In conclusion, we present a unique and challenging case of MCL without cyclin D1 or CD5, but with an expression of CD10 and SOX11, along with t(11;14). Pathologists should explicitly consider the blastoid variant of MCL when dealing with mature B-cell neoplasms with blastoid morphology in adults, and utilize a broad panel of ancillary studies, including FISH and SOX11.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"15 4","pages":"592-596"},"PeriodicalIF":1.2000,"publicationDate":"2023-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594516/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Push to Consider Mantle Cell Lymphoma in Adults with Leukemia/Lymphoma with Blastoid Morphology.\",\"authors\":\"Nkechi Arinze, Nivin Omar, Amany Keruakous, Ravindra Kolhe, Natasha Savage\",\"doi\":\"10.3390/hematolrep15040061\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Mantle cell lymphoma (MCL) is an intermediate-grade B-cell lymphoma, representing 2.8% of all non-Hodgkin lymphomas in the US. It is associated with t(11;14)(q13; q23), which leads to the overexpression of cyclin D1, consequently promoting cell proliferation. MCL usually expresses CD19, CD20, CD43, surface immunoglobulins, FMC7, BCL2, cyclin D1, CD5, and SOX11. Herein is a case of a 67-year-old male, referred to our facility with shortness of breath, anemia (hemoglobin of 5.3 g/dL), thrombocytopenia (12 × 10<sup>9</sup>/L), and leukocytosis (283 × 10<sup>9</sup>/L). A peripheral blood smear showed marked lymphocytosis with blastoid morphology. Morphologic examination of the bone marrow biopsy revealed a diffuse sheet of blastoid cells expressing CD20 and CD10, but without CD5 or cyclin D1. Given these features, a differential diagnosis of diffuse large B-cell lymphoma (DLBCL) with germinal center derivation, high-grade follicular lymphoma, and Burkitt lymphoma was considered, with the latter not favored due to morphology. Additional studies revealed positive SOX11, and fluorescence in situ hybridization (FISH) studies detected t(11;14). These additional studies supported diagnosis of the blastoid variant of MCL. In conclusion, we present a unique and challenging case of MCL without cyclin D1 or CD5, but with an expression of CD10 and SOX11, along with t(11;14). Pathologists should explicitly consider the blastoid variant of MCL when dealing with mature B-cell neoplasms with blastoid morphology in adults, and utilize a broad panel of ancillary studies, including FISH and SOX11.</p>\",\"PeriodicalId\":12829,\"journal\":{\"name\":\"Hematology Reports\",\"volume\":\"15 4\",\"pages\":\"592-596\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-10-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594516/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematology Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/hematolrep15040061\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep15040061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
A Push to Consider Mantle Cell Lymphoma in Adults with Leukemia/Lymphoma with Blastoid Morphology.
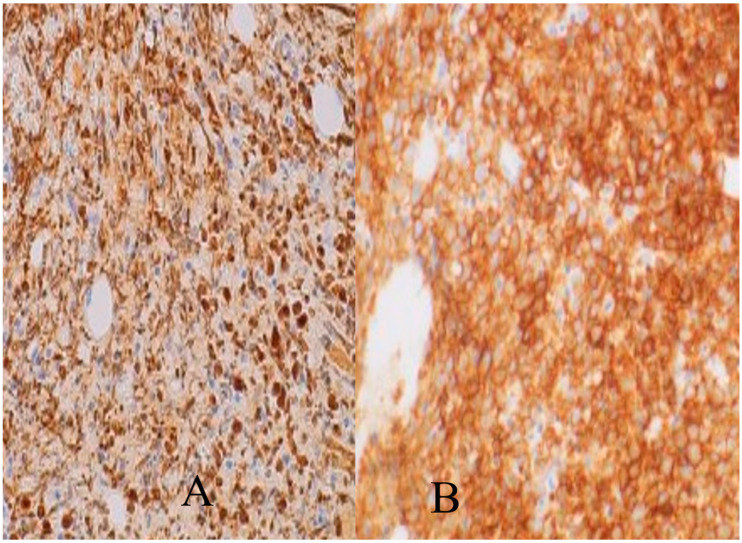
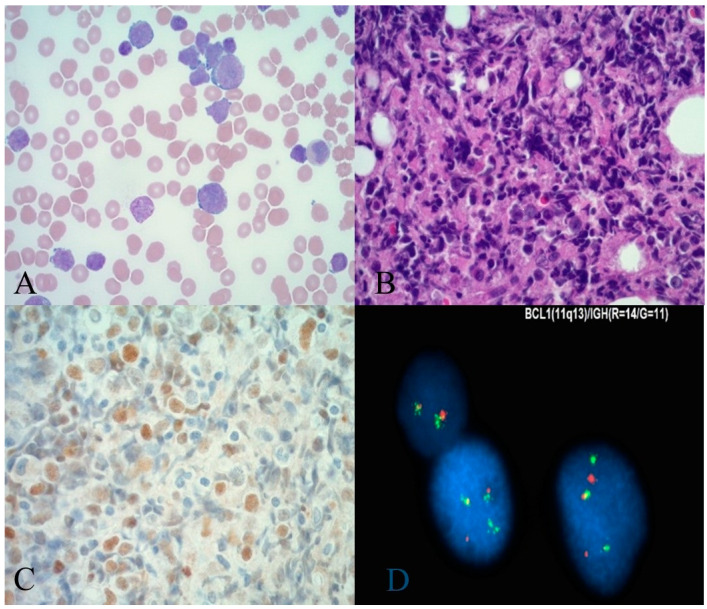
Mantle cell lymphoma (MCL) is an intermediate-grade B-cell lymphoma, representing 2.8% of all non-Hodgkin lymphomas in the US. It is associated with t(11;14)(q13; q23), which leads to the overexpression of cyclin D1, consequently promoting cell proliferation. MCL usually expresses CD19, CD20, CD43, surface immunoglobulins, FMC7, BCL2, cyclin D1, CD5, and SOX11. Herein is a case of a 67-year-old male, referred to our facility with shortness of breath, anemia (hemoglobin of 5.3 g/dL), thrombocytopenia (12 × 109/L), and leukocytosis (283 × 109/L). A peripheral blood smear showed marked lymphocytosis with blastoid morphology. Morphologic examination of the bone marrow biopsy revealed a diffuse sheet of blastoid cells expressing CD20 and CD10, but without CD5 or cyclin D1. Given these features, a differential diagnosis of diffuse large B-cell lymphoma (DLBCL) with germinal center derivation, high-grade follicular lymphoma, and Burkitt lymphoma was considered, with the latter not favored due to morphology. Additional studies revealed positive SOX11, and fluorescence in situ hybridization (FISH) studies detected t(11;14). These additional studies supported diagnosis of the blastoid variant of MCL. In conclusion, we present a unique and challenging case of MCL without cyclin D1 or CD5, but with an expression of CD10 and SOX11, along with t(11;14). Pathologists should explicitly consider the blastoid variant of MCL when dealing with mature B-cell neoplasms with blastoid morphology in adults, and utilize a broad panel of ancillary studies, including FISH and SOX11.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


