{"title":"内镜下乳头状球囊扩张术治疗有症状的括约肌切开术后狭窄","authors":"Vincent Zimmer","doi":"10.1002/aid2.13335","DOIUrl":null,"url":null,"abstract":"<p>Post-sphincterotomy stricture is among the more uncommon long-term complications of preceeding endoscopic retrograde cholangiopancreatography (ERCP) including endoscopic sphincterotomy.<span><sup>1</sup></span> Overall, its incidence is estimated at up to 5% in long-term follow-up, warranting revision ERCP. In lack of a standard revision procedure, endoscopic treatment warrants individualization according to patient- (anatomy-directed) and operator-related (experience, etc.) factors to appropriately choose for example, among re-do papillotomy, balloon dilation and/or temporary metal or multiple plastic stenting.<span><sup>2, 3</sup></span> Specifically, re-do cutting translates into higher risks of bleeding and/or perforation, while stenting and/or dilation is associated with higher post-ERCP pancreatitis (PEP) risks, such that intensified PEP prophylaxis is indicated, as was the case in this 45-year-old female with a symptomatic post-sphincterotomy stricture.<span><sup>4</sup></span> The distinct selection of the revision procedure has to be taken into account aspects of duodenal anatomy (qualifying or not for a safe re-do papillotomy), severity and length of stricture (implying candidacy for stent treatment) as well as individual and institutional experience. The current patient had undergone index ERCP 3 years earlier elsewhere including endoscopic papillotomy to allow for extraction of bile duct stones. The recent ERCP was indicated due to biliary type-pain and elevated cholestasis parameters in association with common bile duct (CBD) dilation on abdominal ultrasound. Duodenoscopy indicated an excentric and severely shrunken biliary orifice post-sphincterotomy without adequate safety plane for re-do papillotomy (no intraduodenal bile duct segment) (Figure 1). After deep-biliary cannulation, a cholangiogram was performed with CBD diameter up to 14 mm with reduced contrast media clearance. After insertion of a 35″ hydrophilic-tip guidewire, endoscopic papillary balloon dilation (EPBD) up to 10 mm was performed (Supplementary Video). The post-interventional course was uncomplicated with complete pain and cholestasis resolution, which was maintained throughout the follow-up period of 1 year.</p><p>The author declares no conflict of interest.</p><p>Ethical approval was waived (clinical routine case); informed consent has been obtained.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"10 3","pages":"193-194"},"PeriodicalIF":0.4000,"publicationDate":"2022-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13335","citationCount":"0","resultStr":"{\"title\":\"Endoscopic papillary balloon dilation for revision of a symptomatic post-sphincterotomy stricture\",\"authors\":\"Vincent Zimmer\",\"doi\":\"10.1002/aid2.13335\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Post-sphincterotomy stricture is among the more uncommon long-term complications of preceeding endoscopic retrograde cholangiopancreatography (ERCP) including endoscopic sphincterotomy.<span><sup>1</sup></span> Overall, its incidence is estimated at up to 5% in long-term follow-up, warranting revision ERCP. In lack of a standard revision procedure, endoscopic treatment warrants individualization according to patient- (anatomy-directed) and operator-related (experience, etc.) factors to appropriately choose for example, among re-do papillotomy, balloon dilation and/or temporary metal or multiple plastic stenting.<span><sup>2, 3</sup></span> Specifically, re-do cutting translates into higher risks of bleeding and/or perforation, while stenting and/or dilation is associated with higher post-ERCP pancreatitis (PEP) risks, such that intensified PEP prophylaxis is indicated, as was the case in this 45-year-old female with a symptomatic post-sphincterotomy stricture.<span><sup>4</sup></span> The distinct selection of the revision procedure has to be taken into account aspects of duodenal anatomy (qualifying or not for a safe re-do papillotomy), severity and length of stricture (implying candidacy for stent treatment) as well as individual and institutional experience. The current patient had undergone index ERCP 3 years earlier elsewhere including endoscopic papillotomy to allow for extraction of bile duct stones. The recent ERCP was indicated due to biliary type-pain and elevated cholestasis parameters in association with common bile duct (CBD) dilation on abdominal ultrasound. Duodenoscopy indicated an excentric and severely shrunken biliary orifice post-sphincterotomy without adequate safety plane for re-do papillotomy (no intraduodenal bile duct segment) (Figure 1). After deep-biliary cannulation, a cholangiogram was performed with CBD diameter up to 14 mm with reduced contrast media clearance. After insertion of a 35″ hydrophilic-tip guidewire, endoscopic papillary balloon dilation (EPBD) up to 10 mm was performed (Supplementary Video). The post-interventional course was uncomplicated with complete pain and cholestasis resolution, which was maintained throughout the follow-up period of 1 year.</p><p>The author declares no conflict of interest.</p><p>Ethical approval was waived (clinical routine case); informed consent has been obtained.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"10 3\",\"pages\":\"193-194\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2022-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13335\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13335\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13335","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Endoscopic papillary balloon dilation for revision of a symptomatic post-sphincterotomy stricture
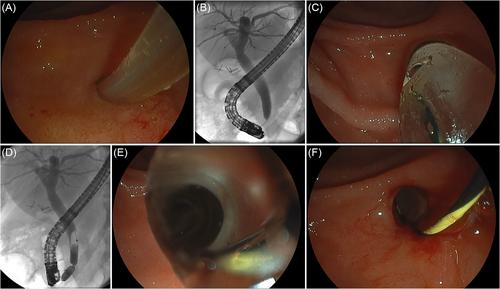
Post-sphincterotomy stricture is among the more uncommon long-term complications of preceeding endoscopic retrograde cholangiopancreatography (ERCP) including endoscopic sphincterotomy.1 Overall, its incidence is estimated at up to 5% in long-term follow-up, warranting revision ERCP. In lack of a standard revision procedure, endoscopic treatment warrants individualization according to patient- (anatomy-directed) and operator-related (experience, etc.) factors to appropriately choose for example, among re-do papillotomy, balloon dilation and/or temporary metal or multiple plastic stenting.2, 3 Specifically, re-do cutting translates into higher risks of bleeding and/or perforation, while stenting and/or dilation is associated with higher post-ERCP pancreatitis (PEP) risks, such that intensified PEP prophylaxis is indicated, as was the case in this 45-year-old female with a symptomatic post-sphincterotomy stricture.4 The distinct selection of the revision procedure has to be taken into account aspects of duodenal anatomy (qualifying or not for a safe re-do papillotomy), severity and length of stricture (implying candidacy for stent treatment) as well as individual and institutional experience. The current patient had undergone index ERCP 3 years earlier elsewhere including endoscopic papillotomy to allow for extraction of bile duct stones. The recent ERCP was indicated due to biliary type-pain and elevated cholestasis parameters in association with common bile duct (CBD) dilation on abdominal ultrasound. Duodenoscopy indicated an excentric and severely shrunken biliary orifice post-sphincterotomy without adequate safety plane for re-do papillotomy (no intraduodenal bile duct segment) (Figure 1). After deep-biliary cannulation, a cholangiogram was performed with CBD diameter up to 14 mm with reduced contrast media clearance. After insertion of a 35″ hydrophilic-tip guidewire, endoscopic papillary balloon dilation (EPBD) up to 10 mm was performed (Supplementary Video). The post-interventional course was uncomplicated with complete pain and cholestasis resolution, which was maintained throughout the follow-up period of 1 year.
The author declares no conflict of interest.
Ethical approval was waived (clinical routine case); informed consent has been obtained.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


