{"title":"家族性感冒自身炎症综合征与多发性硬化","authors":"Syed Basharat Ali, Debajyoti Chaudhuri, Deborah Field, Pravin Hissaria","doi":"10.1111/cen3.12697","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Cryopyrin-associated periodic syndrome (CAPS) is an autoinflammatory disorder with a spectrum ranging from the milder familial cold auto-inflammatory syndrome (FCAS) phenotype to the more severe Muckle–Wells Syndrome. Although headaches are the most common neurological symptoms, neuroinflammatory diseases such as multiple sclerosis (MS) have only been reported in the more severe phenotypes.</p>\n </section>\n \n <section>\n \n <h3> Case Presentation</h3>\n \n <p>We describe a 43-year-old male diagnosed with relapse-remitting MS who developed cold-induced arthralgias and urticaria. He initially presented with facial numbness and arthralgias in his late teenage years, and brain magnetic resonance imaging (MRI) demonstrated multiple lesions with periventricular white matter extension. Oligoclonal bands were detected in the cerebrospinal fluid (CSF). Symptoms gradually improved, and a decade later he presented with numbness at upper limbs and tongue. Brain and spine MRI showed new lesions, but CSF was unremarkable. He was started on interferon β-1a with symptomatic improvement until another flare around 13 years later. Treatment was changed to dimethyl fumarate. During this hospitalization, urticaria was problematic and particularly associated with cold temperatures. This raised suspicion for possible CAPS and subsequently confirmed with an A439V mutation in the <i>NLRP3</i> gene, consistent with FCAS. Anakinra was started but was not tolerated because of localized reactions despite desensitization. His serum amyloid A was mildly elevated at 9 mg/L (reference range 0–6). He remains stable from a neurological perspective, including imaging, and continues dimethyl fumarate.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>To date, FCAS and possible association with MS has not been described. The case raises challenges in the diagnosis of concurrent disease processes. It also highlights that neurological sequelae should be considered in all spectrums of CAPS, and distinctions with MS should be made where possible.</p>\n </section>\n </div>","PeriodicalId":10193,"journal":{"name":"Clinical and Experimental Neuroimmunology","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2022-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen3.12697","citationCount":"1","resultStr":"{\"title\":\"Familial cold autoinflammatory syndrome and multiple sclerosis\",\"authors\":\"Syed Basharat Ali, Debajyoti Chaudhuri, Deborah Field, Pravin Hissaria\",\"doi\":\"10.1111/cen3.12697\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Cryopyrin-associated periodic syndrome (CAPS) is an autoinflammatory disorder with a spectrum ranging from the milder familial cold auto-inflammatory syndrome (FCAS) phenotype to the more severe Muckle–Wells Syndrome. Although headaches are the most common neurological symptoms, neuroinflammatory diseases such as multiple sclerosis (MS) have only been reported in the more severe phenotypes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Case Presentation</h3>\\n \\n <p>We describe a 43-year-old male diagnosed with relapse-remitting MS who developed cold-induced arthralgias and urticaria. He initially presented with facial numbness and arthralgias in his late teenage years, and brain magnetic resonance imaging (MRI) demonstrated multiple lesions with periventricular white matter extension. Oligoclonal bands were detected in the cerebrospinal fluid (CSF). Symptoms gradually improved, and a decade later he presented with numbness at upper limbs and tongue. Brain and spine MRI showed new lesions, but CSF was unremarkable. He was started on interferon β-1a with symptomatic improvement until another flare around 13 years later. Treatment was changed to dimethyl fumarate. During this hospitalization, urticaria was problematic and particularly associated with cold temperatures. This raised suspicion for possible CAPS and subsequently confirmed with an A439V mutation in the <i>NLRP3</i> gene, consistent with FCAS. Anakinra was started but was not tolerated because of localized reactions despite desensitization. His serum amyloid A was mildly elevated at 9 mg/L (reference range 0–6). He remains stable from a neurological perspective, including imaging, and continues dimethyl fumarate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>To date, FCAS and possible association with MS has not been described. The case raises challenges in the diagnosis of concurrent disease processes. It also highlights that neurological sequelae should be considered in all spectrums of CAPS, and distinctions with MS should be made where possible.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10193,\"journal\":{\"name\":\"Clinical and Experimental Neuroimmunology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen3.12697\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Neuroimmunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cen3.12697\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Immunology and Microbiology\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Neuroimmunology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cen3.12697","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Immunology and Microbiology","Score":null,"Total":0}
Familial cold autoinflammatory syndrome and multiple sclerosis
Background
Cryopyrin-associated periodic syndrome (CAPS) is an autoinflammatory disorder with a spectrum ranging from the milder familial cold auto-inflammatory syndrome (FCAS) phenotype to the more severe Muckle–Wells Syndrome. Although headaches are the most common neurological symptoms, neuroinflammatory diseases such as multiple sclerosis (MS) have only been reported in the more severe phenotypes.
Case Presentation
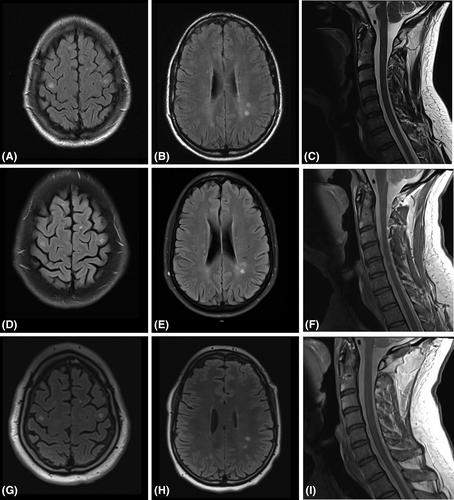
We describe a 43-year-old male diagnosed with relapse-remitting MS who developed cold-induced arthralgias and urticaria. He initially presented with facial numbness and arthralgias in his late teenage years, and brain magnetic resonance imaging (MRI) demonstrated multiple lesions with periventricular white matter extension. Oligoclonal bands were detected in the cerebrospinal fluid (CSF). Symptoms gradually improved, and a decade later he presented with numbness at upper limbs and tongue. Brain and spine MRI showed new lesions, but CSF was unremarkable. He was started on interferon β-1a with symptomatic improvement until another flare around 13 years later. Treatment was changed to dimethyl fumarate. During this hospitalization, urticaria was problematic and particularly associated with cold temperatures. This raised suspicion for possible CAPS and subsequently confirmed with an A439V mutation in the NLRP3 gene, consistent with FCAS. Anakinra was started but was not tolerated because of localized reactions despite desensitization. His serum amyloid A was mildly elevated at 9 mg/L (reference range 0–6). He remains stable from a neurological perspective, including imaging, and continues dimethyl fumarate.
Conclusions
To date, FCAS and possible association with MS has not been described. The case raises challenges in the diagnosis of concurrent disease processes. It also highlights that neurological sequelae should be considered in all spectrums of CAPS, and distinctions with MS should be made where possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


