Mohammed Abdulhaleem, Hannah Johnston, Ralph D'Agostino, Claire Lanier, Christina K Cramer, Pierre Triozzi, Hui-Wen Lo, Fei Xing, Wencheng Li, Christopher Whitlow, Jaclyn J White, Stephen B Tatter, Adrian W Laxton, Jing Su, Michael D Chan, Jimmy Ruiz
{"title":"立体定向放射手术和免疫治疗联合治疗黑色素瘤脑转移的失败结果模式","authors":"Mohammed Abdulhaleem, Hannah Johnston, Ralph D'Agostino, Claire Lanier, Christina K Cramer, Pierre Triozzi, Hui-Wen Lo, Fei Xing, Wencheng Li, Christopher Whitlow, Jaclyn J White, Stephen B Tatter, Adrian W Laxton, Jing Su, Michael D Chan, Jimmy Ruiz","doi":"10.1227/neuprac.0000000000000026","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous series have demonstrated central nervous system activity for immune checkpoint inhibitors (ICIs) and shown improved local control between stereotactic radiosurgery (SRS) and ICI for lung cancer brain metastases.</p><p><strong>Objective: </strong>To assess whether the addition of ICI to SRS for melanoma brain metastasis improves outcomes when compared with historical control group treated in the era before ICI availability.</p><p><strong>Methods: </strong>In this single institution retrospective series, outcomes of 24 patients with melanoma receiving concurrent ICI and SRS were compared with 111 historical controls treated before ICI era. Overall survival (OS) was estimated using the Kaplan-Meier method. Cumulative incidence of local and distant failures was estimated using a competing risk model that accounted for baseline differences using propensity score adjustments.</p><p><strong>Results: </strong>The median OS time was improved in patients receiving ICI compared with the historical control group (17.6 vs 6.6 months, hazard ratio [HR] = 0.056, <i>P</i> = .0005). Cumulative incidence at 1 year for local failure in the historical control and ICI groups was approximately 12.5% and 6.5%, respectively (HR = 0.25, <i>P</i> = .19), while cumulative incidence of distant brain failure in the historical control and ICI groups was approximately 48% and 28%, respectively (HR = 0.326, <i>P</i> = .015).</p><p><strong>Conclusion: </strong>Distant brain failure and OS were improved in patients receiving concurrent ICI with SRS compared with historical controls. Local failure trended in the same direction; however, owing to small sample size, this did not reach statistical significance. While these data remain to be validated, they suggest that patients with brain metastasis may benefit from concurrent use of ICI with SRS.</p>","PeriodicalId":93342,"journal":{"name":"Neurosurgery open","volume":" ","pages":"e00026"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809996/pdf/","citationCount":"0","resultStr":"{\"title\":\"Patterns of Failure Outcomes for Combination of Stereotactic Radiosurgery and Immunotherapy for Melanoma Brain Metastases.\",\"authors\":\"Mohammed Abdulhaleem, Hannah Johnston, Ralph D'Agostino, Claire Lanier, Christina K Cramer, Pierre Triozzi, Hui-Wen Lo, Fei Xing, Wencheng Li, Christopher Whitlow, Jaclyn J White, Stephen B Tatter, Adrian W Laxton, Jing Su, Michael D Chan, Jimmy Ruiz\",\"doi\":\"10.1227/neuprac.0000000000000026\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Previous series have demonstrated central nervous system activity for immune checkpoint inhibitors (ICIs) and shown improved local control between stereotactic radiosurgery (SRS) and ICI for lung cancer brain metastases.</p><p><strong>Objective: </strong>To assess whether the addition of ICI to SRS for melanoma brain metastasis improves outcomes when compared with historical control group treated in the era before ICI availability.</p><p><strong>Methods: </strong>In this single institution retrospective series, outcomes of 24 patients with melanoma receiving concurrent ICI and SRS were compared with 111 historical controls treated before ICI era. Overall survival (OS) was estimated using the Kaplan-Meier method. Cumulative incidence of local and distant failures was estimated using a competing risk model that accounted for baseline differences using propensity score adjustments.</p><p><strong>Results: </strong>The median OS time was improved in patients receiving ICI compared with the historical control group (17.6 vs 6.6 months, hazard ratio [HR] = 0.056, <i>P</i> = .0005). Cumulative incidence at 1 year for local failure in the historical control and ICI groups was approximately 12.5% and 6.5%, respectively (HR = 0.25, <i>P</i> = .19), while cumulative incidence of distant brain failure in the historical control and ICI groups was approximately 48% and 28%, respectively (HR = 0.326, <i>P</i> = .015).</p><p><strong>Conclusion: </strong>Distant brain failure and OS were improved in patients receiving concurrent ICI with SRS compared with historical controls. Local failure trended in the same direction; however, owing to small sample size, this did not reach statistical significance. While these data remain to be validated, they suggest that patients with brain metastasis may benefit from concurrent use of ICI with SRS.</p>\",\"PeriodicalId\":93342,\"journal\":{\"name\":\"Neurosurgery open\",\"volume\":\" \",\"pages\":\"e00026\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809996/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurosurgery open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1227/neuprac.0000000000000026\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgery open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1227/neuprac.0000000000000026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:先前的系列研究已经证明免疫检查点抑制剂(ICIs)对中枢神经系统有活性,并显示立体定向放射手术(SRS)和ICI治疗肺癌脑转移的局部控制改善。目的:评估在SRS中加入ICI治疗黑素瘤脑转移是否能改善预后,与在ICI可用前治疗的历史对照组相比。方法:在这个单机构回顾性系列研究中,将24例同时接受ICI和SRS治疗的黑色素瘤患者的结果与111例在ICI时代之前接受治疗的历史对照进行比较。采用Kaplan-Meier法估计总生存期(OS)。使用竞争风险模型估计本地和远程失败的累积发生率,该模型使用倾向评分调整来解释基线差异。结果:与历史对照组相比,ICI患者的中位OS时间有所改善(17.6个月vs 6.6个月,风险比[HR] = 0.056, P = 0.0005)。历史对照组和ICI组1年累积局部脑衰竭发生率分别约为12.5%和6.5% (HR = 0.25, P = 0.19),而历史对照组和ICI组1年累积远端脑衰竭发生率分别约为48%和28% (HR = 0.326, P = 0.015)。结论:与历史对照组相比,同时接受ICI和SRS的患者远端脑衰竭和OS得到改善。局部破坏趋势相同;但由于样本量小,没有达到统计学意义。虽然这些数据仍有待验证,但它们表明脑转移患者可能受益于同时使用ICI和SRS。
Patterns of Failure Outcomes for Combination of Stereotactic Radiosurgery and Immunotherapy for Melanoma Brain Metastases.
Background: Previous series have demonstrated central nervous system activity for immune checkpoint inhibitors (ICIs) and shown improved local control between stereotactic radiosurgery (SRS) and ICI for lung cancer brain metastases.
Objective: To assess whether the addition of ICI to SRS for melanoma brain metastasis improves outcomes when compared with historical control group treated in the era before ICI availability.
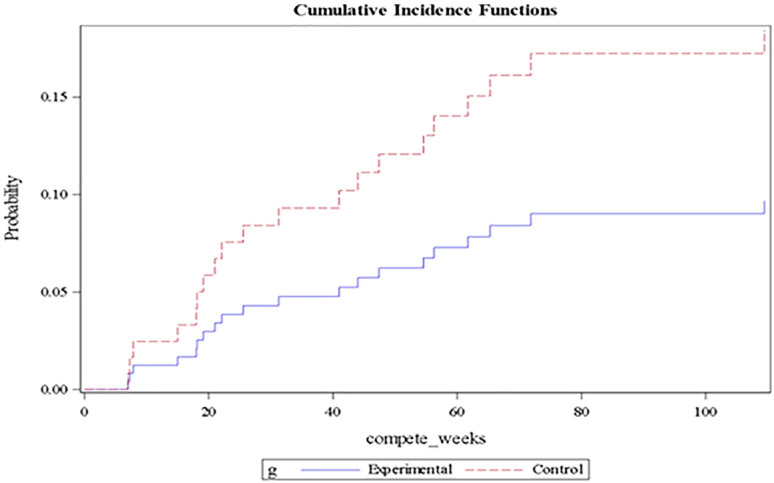
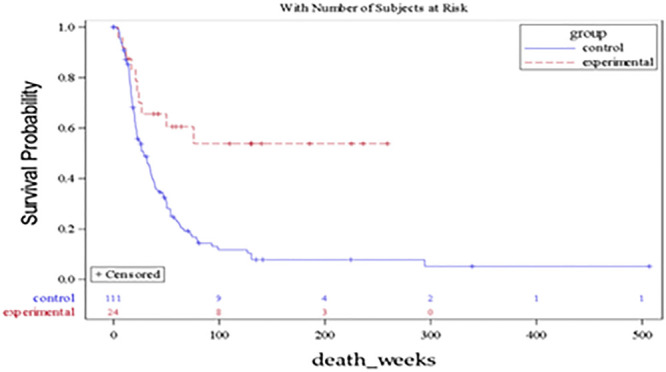
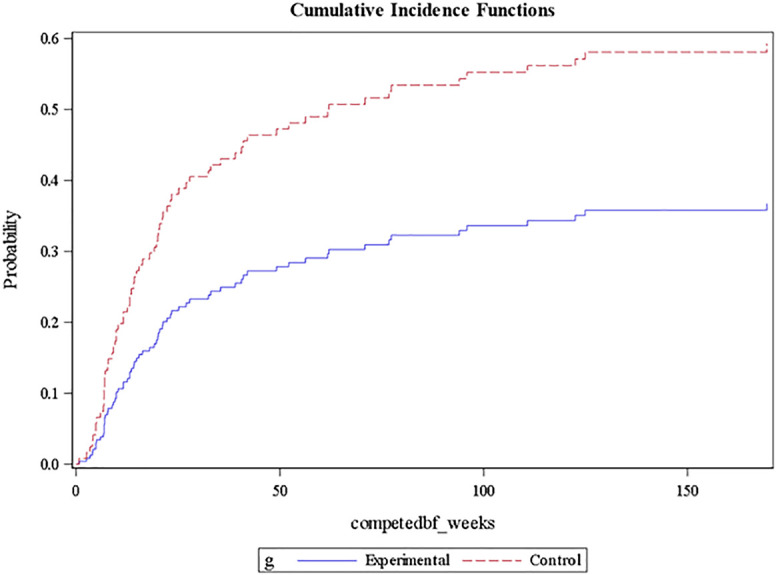
Methods: In this single institution retrospective series, outcomes of 24 patients with melanoma receiving concurrent ICI and SRS were compared with 111 historical controls treated before ICI era. Overall survival (OS) was estimated using the Kaplan-Meier method. Cumulative incidence of local and distant failures was estimated using a competing risk model that accounted for baseline differences using propensity score adjustments.
Results: The median OS time was improved in patients receiving ICI compared with the historical control group (17.6 vs 6.6 months, hazard ratio [HR] = 0.056, P = .0005). Cumulative incidence at 1 year for local failure in the historical control and ICI groups was approximately 12.5% and 6.5%, respectively (HR = 0.25, P = .19), while cumulative incidence of distant brain failure in the historical control and ICI groups was approximately 48% and 28%, respectively (HR = 0.326, P = .015).
Conclusion: Distant brain failure and OS were improved in patients receiving concurrent ICI with SRS compared with historical controls. Local failure trended in the same direction; however, owing to small sample size, this did not reach statistical significance. While these data remain to be validated, they suggest that patients with brain metastasis may benefit from concurrent use of ICI with SRS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


