Min-Jie Yang, Ming-Lun Han, Wei-Ti Chang, Hsiu-Po Wang
{"title":"胰腺粘液性囊腺瘤模拟胰腺假性囊肿","authors":"Min-Jie Yang, Ming-Lun Han, Wei-Ti Chang, Hsiu-Po Wang","doi":"10.1002/aid2.13340","DOIUrl":null,"url":null,"abstract":"<p>A 37-year-old woman with a history of acute pancreatitis underwent abdominal ultrasound, which revealed a cystic lesion at the pancreatic tail. Ultrasound-guided cyst aspiration was performed, and the fluid analysis showed a high level of carcinoembryonic antigen (CEA, 1470 ng/mL), amylase (31 835 U/L) and lipase (102 410 U/L). Further abdominal computed tomography (CT) revealed a 6.3-cm unilocular cystic lesion with a well-defined thin wall, which can be enhanced by contrast-enhanced endoscopic ultrasound. Magnetic resonance cholangiopancreatography (MRCP) was then arranged and revealed the communication between the cyst and the main pancreatic duct (Figure 1). Pancreatic pseudocyst was initially diagnosed, and transpapillary endoscopic retrograde pancreatic stent drainage was performed for symptomatic relief.</p><p>Three months after the stent implantation, CT showed a significantly shrunken pancreatic cyst. One month after removal of the plastic stent, however, a recurrent pancreatic cyst was revealed by abdominal ultrasound. Thus, fine needle aspiration guided by contrast-enhanced endoscopic ultrasound was performed, and showed a 2.8 cm-in-diameter hypoechoic cystic tumor with a 1.1 cm-in-diameter anechoic region (Figure 2). The CEA level of the cystic fluid was up to 1470 ng/mL; pancreatic mucinous cystadenoma was thus highly suspected. The pathological report after distal pancreatectomy with splenectomy confirmed the cystic lesion as a mucinous cystadenoma in the tail of pancreas with a potential of malignant change.</p><p>The cystic lesion of our patient was initially treated as a pancreatic pseudocyst. However, the discrepancy lies in the lack of obvious risk factors for pancreatitis in this patient, such as alcohol consumption, gallstones, and hypertriglyceridemia. By contrast, pancreatic cystadenomas usually manifest abdominal pain in middle-aged women,<span><sup>1</sup></span> but rarely cause pancreatitis.<span><sup>2</sup></span> Elevated amylase level in serum and aspirated cystic fluid are not observed in most cases of pancreatic cystadenomas.<span><sup>3, 4</sup></span> However, there are few exceptions,<span><sup>2</sup></span> as in our case, where elevated amylase level in the cystic fluid was contributed by its connection to main pancreatic duct, which may activate pancreatic enzyme and trigger acute pancreatitis. In cases of pancreatic cysts with re-expanding after drainage or incomplete drainage, pancreatic cystadenomas should be highly suspected, which should be treated surgically.<span><sup>2, 4</sup></span></p><p>The authors declare no conflicts of interest.</p><p>Written informed consent was obtained from the patient.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"10 4","pages":"257-258"},"PeriodicalIF":0.4000,"publicationDate":"2022-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13340","citationCount":"0","resultStr":"{\"title\":\"Pancreatic mucinous cystadenoma mimicking pancreatic pseudocyst\",\"authors\":\"Min-Jie Yang, Ming-Lun Han, Wei-Ti Chang, Hsiu-Po Wang\",\"doi\":\"10.1002/aid2.13340\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 37-year-old woman with a history of acute pancreatitis underwent abdominal ultrasound, which revealed a cystic lesion at the pancreatic tail. Ultrasound-guided cyst aspiration was performed, and the fluid analysis showed a high level of carcinoembryonic antigen (CEA, 1470 ng/mL), amylase (31 835 U/L) and lipase (102 410 U/L). Further abdominal computed tomography (CT) revealed a 6.3-cm unilocular cystic lesion with a well-defined thin wall, which can be enhanced by contrast-enhanced endoscopic ultrasound. Magnetic resonance cholangiopancreatography (MRCP) was then arranged and revealed the communication between the cyst and the main pancreatic duct (Figure 1). Pancreatic pseudocyst was initially diagnosed, and transpapillary endoscopic retrograde pancreatic stent drainage was performed for symptomatic relief.</p><p>Three months after the stent implantation, CT showed a significantly shrunken pancreatic cyst. One month after removal of the plastic stent, however, a recurrent pancreatic cyst was revealed by abdominal ultrasound. Thus, fine needle aspiration guided by contrast-enhanced endoscopic ultrasound was performed, and showed a 2.8 cm-in-diameter hypoechoic cystic tumor with a 1.1 cm-in-diameter anechoic region (Figure 2). The CEA level of the cystic fluid was up to 1470 ng/mL; pancreatic mucinous cystadenoma was thus highly suspected. The pathological report after distal pancreatectomy with splenectomy confirmed the cystic lesion as a mucinous cystadenoma in the tail of pancreas with a potential of malignant change.</p><p>The cystic lesion of our patient was initially treated as a pancreatic pseudocyst. However, the discrepancy lies in the lack of obvious risk factors for pancreatitis in this patient, such as alcohol consumption, gallstones, and hypertriglyceridemia. By contrast, pancreatic cystadenomas usually manifest abdominal pain in middle-aged women,<span><sup>1</sup></span> but rarely cause pancreatitis.<span><sup>2</sup></span> Elevated amylase level in serum and aspirated cystic fluid are not observed in most cases of pancreatic cystadenomas.<span><sup>3, 4</sup></span> However, there are few exceptions,<span><sup>2</sup></span> as in our case, where elevated amylase level in the cystic fluid was contributed by its connection to main pancreatic duct, which may activate pancreatic enzyme and trigger acute pancreatitis. In cases of pancreatic cysts with re-expanding after drainage or incomplete drainage, pancreatic cystadenomas should be highly suspected, which should be treated surgically.<span><sup>2, 4</sup></span></p><p>The authors declare no conflicts of interest.</p><p>Written informed consent was obtained from the patient.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"10 4\",\"pages\":\"257-258\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2022-08-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13340\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13340\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13340","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
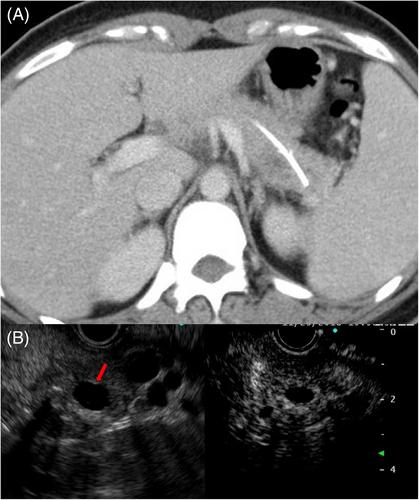
A 37-year-old woman with a history of acute pancreatitis underwent abdominal ultrasound, which revealed a cystic lesion at the pancreatic tail. Ultrasound-guided cyst aspiration was performed, and the fluid analysis showed a high level of carcinoembryonic antigen (CEA, 1470 ng/mL), amylase (31 835 U/L) and lipase (102 410 U/L). Further abdominal computed tomography (CT) revealed a 6.3-cm unilocular cystic lesion with a well-defined thin wall, which can be enhanced by contrast-enhanced endoscopic ultrasound. Magnetic resonance cholangiopancreatography (MRCP) was then arranged and revealed the communication between the cyst and the main pancreatic duct (Figure 1). Pancreatic pseudocyst was initially diagnosed, and transpapillary endoscopic retrograde pancreatic stent drainage was performed for symptomatic relief.
Three months after the stent implantation, CT showed a significantly shrunken pancreatic cyst. One month after removal of the plastic stent, however, a recurrent pancreatic cyst was revealed by abdominal ultrasound. Thus, fine needle aspiration guided by contrast-enhanced endoscopic ultrasound was performed, and showed a 2.8 cm-in-diameter hypoechoic cystic tumor with a 1.1 cm-in-diameter anechoic region (Figure 2). The CEA level of the cystic fluid was up to 1470 ng/mL; pancreatic mucinous cystadenoma was thus highly suspected. The pathological report after distal pancreatectomy with splenectomy confirmed the cystic lesion as a mucinous cystadenoma in the tail of pancreas with a potential of malignant change.
The cystic lesion of our patient was initially treated as a pancreatic pseudocyst. However, the discrepancy lies in the lack of obvious risk factors for pancreatitis in this patient, such as alcohol consumption, gallstones, and hypertriglyceridemia. By contrast, pancreatic cystadenomas usually manifest abdominal pain in middle-aged women,1 but rarely cause pancreatitis.2 Elevated amylase level in serum and aspirated cystic fluid are not observed in most cases of pancreatic cystadenomas.3, 4 However, there are few exceptions,2 as in our case, where elevated amylase level in the cystic fluid was contributed by its connection to main pancreatic duct, which may activate pancreatic enzyme and trigger acute pancreatitis. In cases of pancreatic cysts with re-expanding after drainage or incomplete drainage, pancreatic cystadenomas should be highly suspected, which should be treated surgically.2, 4
The authors declare no conflicts of interest.
Written informed consent was obtained from the patient.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


