Jing Liang Ho, Edric J. H. Hee, Stephen K. K. Tsao, Christopher T. W. Chia, Cora Yuk-Ping Chau
{"title":"常用处方药引起的结肠损伤","authors":"Jing Liang Ho, Edric J. H. Hee, Stephen K. K. Tsao, Christopher T. W. Chia, Cora Yuk-Ping Chau","doi":"10.1002/aid2.13360","DOIUrl":null,"url":null,"abstract":"<p>A 54-year-old lady was hospitalized for pericardial tamponade. An urgent pericardial drainage was performed. She was also noted to have acute kidney injury complicated by severe hyperkalemia of 7.0 mmol/L. The hyperkalemia was corrected with multiple doses of oral sodium polystyrene sulfonate (SPS) as well as a combination of intravenous insulin and dextrose injection, followed by 48 h of continuous renal replacement therapy. After 10 days, she developed fresh rectal bleeding with mild tachycardia. After stabilizing the patient including blood products transfusion, bidirectional gastrointestinal endoscopy was performed. The upper gastrointestinal endoscopy was unremarkable.</p><p>Colonoscopy revealed numerous necrotic ulcers involving the cecum (Figure 1A), and clean-based ulcers in the sigmoid colon (Figure 1B). The rest of the colon mucosa was normal. Histology of the colonic biopsies showed fragments of polygonal basophilic crystals with mosaic pattern at the ulcer base (Figure 2A). Colon ischemia was an important differential diagnosis; however, the finding of some of these crystals being surrounded by granulation tissue and inflammatory infiltrate (Figure 2B) supported the diagnosis of SPS-induced colon injury. Pseudomembranous colitis, viral inclusions, crypt distortion, crypt abscess, or granuloma were not seen, making other differential diagnoses, such as infective colitis with ulcers and inflammatory bowel disease, not likely.</p><p>SPS is a commonly used cation exchange resin in the management of hyperkalemia. In a large population-level matched cohort study, SPS was found to be associated with higher risk of serious adverse gastrointestinal events.<span><sup>1</sup></span> SPS-related adverse gastrointestinal event such as ulcer, necrosis, or perforation, although uncommon, can occur to any segment of the gastrointestinal tract, with colon being the most common site. Irrespective of the location of the injury in the gastrointestinal tract, the mortality rate remained high and was found to be 20.7% in a systemic review.<span><sup>2</sup></span></p><p>The diagnosis of SPS-induced gastrointestinal injury can be accurately made when there is a history of SPS exposure with temporal relationship to the symptom onset, together with histological evidence of SPS crystals in the biopsy sample. Risk factors include chronic kidney disease, uremia, solid organ transplantation and immunosuppressive therapy, postoperative status, hypotension, ileus, and opioid use.<span><sup>3</sup></span> Clinicians ought to exercise prudence in prescribing SPS, especially in patients who are critically ill with multiple risk factors. In such cases, newer gastrointestinal potassium binder like sodium zirconium cyclosilicate will likely be a safer option.</p><p>The authors declare no conflicts of interest.</p><p>Informed consent was obtained. Ethics committee approval is not necessary locally as this is a simple case report. Nonetheless, the principles outlined in the Declaration of Helsinki are strictly complied to.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 1","pages":"51-52"},"PeriodicalIF":0.4000,"publicationDate":"2023-01-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13360","citationCount":"0","resultStr":"{\"title\":\"Colonic injury from a commonly prescribed medication\",\"authors\":\"Jing Liang Ho, Edric J. H. Hee, Stephen K. K. Tsao, Christopher T. W. Chia, Cora Yuk-Ping Chau\",\"doi\":\"10.1002/aid2.13360\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 54-year-old lady was hospitalized for pericardial tamponade. An urgent pericardial drainage was performed. She was also noted to have acute kidney injury complicated by severe hyperkalemia of 7.0 mmol/L. The hyperkalemia was corrected with multiple doses of oral sodium polystyrene sulfonate (SPS) as well as a combination of intravenous insulin and dextrose injection, followed by 48 h of continuous renal replacement therapy. After 10 days, she developed fresh rectal bleeding with mild tachycardia. After stabilizing the patient including blood products transfusion, bidirectional gastrointestinal endoscopy was performed. The upper gastrointestinal endoscopy was unremarkable.</p><p>Colonoscopy revealed numerous necrotic ulcers involving the cecum (Figure 1A), and clean-based ulcers in the sigmoid colon (Figure 1B). The rest of the colon mucosa was normal. Histology of the colonic biopsies showed fragments of polygonal basophilic crystals with mosaic pattern at the ulcer base (Figure 2A). Colon ischemia was an important differential diagnosis; however, the finding of some of these crystals being surrounded by granulation tissue and inflammatory infiltrate (Figure 2B) supported the diagnosis of SPS-induced colon injury. Pseudomembranous colitis, viral inclusions, crypt distortion, crypt abscess, or granuloma were not seen, making other differential diagnoses, such as infective colitis with ulcers and inflammatory bowel disease, not likely.</p><p>SPS is a commonly used cation exchange resin in the management of hyperkalemia. In a large population-level matched cohort study, SPS was found to be associated with higher risk of serious adverse gastrointestinal events.<span><sup>1</sup></span> SPS-related adverse gastrointestinal event such as ulcer, necrosis, or perforation, although uncommon, can occur to any segment of the gastrointestinal tract, with colon being the most common site. Irrespective of the location of the injury in the gastrointestinal tract, the mortality rate remained high and was found to be 20.7% in a systemic review.<span><sup>2</sup></span></p><p>The diagnosis of SPS-induced gastrointestinal injury can be accurately made when there is a history of SPS exposure with temporal relationship to the symptom onset, together with histological evidence of SPS crystals in the biopsy sample. Risk factors include chronic kidney disease, uremia, solid organ transplantation and immunosuppressive therapy, postoperative status, hypotension, ileus, and opioid use.<span><sup>3</sup></span> Clinicians ought to exercise prudence in prescribing SPS, especially in patients who are critically ill with multiple risk factors. In such cases, newer gastrointestinal potassium binder like sodium zirconium cyclosilicate will likely be a safer option.</p><p>The authors declare no conflicts of interest.</p><p>Informed consent was obtained. Ethics committee approval is not necessary locally as this is a simple case report. Nonetheless, the principles outlined in the Declaration of Helsinki are strictly complied to.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"11 1\",\"pages\":\"51-52\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2023-01-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13360\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13360\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13360","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Colonic injury from a commonly prescribed medication
A 54-year-old lady was hospitalized for pericardial tamponade. An urgent pericardial drainage was performed. She was also noted to have acute kidney injury complicated by severe hyperkalemia of 7.0 mmol/L. The hyperkalemia was corrected with multiple doses of oral sodium polystyrene sulfonate (SPS) as well as a combination of intravenous insulin and dextrose injection, followed by 48 h of continuous renal replacement therapy. After 10 days, she developed fresh rectal bleeding with mild tachycardia. After stabilizing the patient including blood products transfusion, bidirectional gastrointestinal endoscopy was performed. The upper gastrointestinal endoscopy was unremarkable.
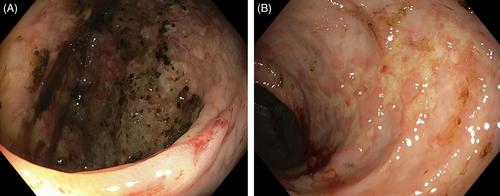
Colonoscopy revealed numerous necrotic ulcers involving the cecum (Figure 1A), and clean-based ulcers in the sigmoid colon (Figure 1B). The rest of the colon mucosa was normal. Histology of the colonic biopsies showed fragments of polygonal basophilic crystals with mosaic pattern at the ulcer base (Figure 2A). Colon ischemia was an important differential diagnosis; however, the finding of some of these crystals being surrounded by granulation tissue and inflammatory infiltrate (Figure 2B) supported the diagnosis of SPS-induced colon injury. Pseudomembranous colitis, viral inclusions, crypt distortion, crypt abscess, or granuloma were not seen, making other differential diagnoses, such as infective colitis with ulcers and inflammatory bowel disease, not likely.
SPS is a commonly used cation exchange resin in the management of hyperkalemia. In a large population-level matched cohort study, SPS was found to be associated with higher risk of serious adverse gastrointestinal events.1 SPS-related adverse gastrointestinal event such as ulcer, necrosis, or perforation, although uncommon, can occur to any segment of the gastrointestinal tract, with colon being the most common site. Irrespective of the location of the injury in the gastrointestinal tract, the mortality rate remained high and was found to be 20.7% in a systemic review.2
The diagnosis of SPS-induced gastrointestinal injury can be accurately made when there is a history of SPS exposure with temporal relationship to the symptom onset, together with histological evidence of SPS crystals in the biopsy sample. Risk factors include chronic kidney disease, uremia, solid organ transplantation and immunosuppressive therapy, postoperative status, hypotension, ileus, and opioid use.3 Clinicians ought to exercise prudence in prescribing SPS, especially in patients who are critically ill with multiple risk factors. In such cases, newer gastrointestinal potassium binder like sodium zirconium cyclosilicate will likely be a safer option.
The authors declare no conflicts of interest.
Informed consent was obtained. Ethics committee approval is not necessary locally as this is a simple case report. Nonetheless, the principles outlined in the Declaration of Helsinki are strictly complied to.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


