Sanket P. Shah, Vivek S. Radhakrishnan, Ganesh S. Jaishetwar, Reghu K. Sukumaran, Jeevan Kumar, Saurabh J. Bhave, Mita Roychowdhury, Sayak Chaudhuri, Deepak K. Mishra, Reena Nair, Shekhar Krishnan, Mammen Chandy
{"title":"高风险血液系统恶性肿瘤移植后环磷酰胺的骨髓清除性单倍体全t细胞造血细胞移植:中等收入环境下的学习曲线弯曲","authors":"Sanket P. Shah, Vivek S. Radhakrishnan, Ganesh S. Jaishetwar, Reghu K. Sukumaran, Jeevan Kumar, Saurabh J. Bhave, Mita Roychowdhury, Sayak Chaudhuri, Deepak K. Mishra, Reena Nair, Shekhar Krishnan, Mammen Chandy","doi":"10.1002/acg2.106","DOIUrl":null,"url":null,"abstract":"<p>Haploidentical peripheral blood hematopoietic cell transplantation has become the preferred alternative donor transplant program in most centers in India, owing to its logistic and cost advantages. This is a retrospective analysis of 59 patients with high-risk hematological malignancies who underwent haploidentical transplant in three different centers, using myeloablative conditioning and unmanipulated stem cell graft. GVHD prophylaxis was post-transplant Cyclophosphamide (PTCy D + 3, D + 4) along with Tacrolimus and Mycophenolate Mofetil (D + 5 onwards). The median CD34 cell dose was 5.8 x 10<sup>6</sup> cells/kg. Neutrophils engrafted in 50 (83%) patients [median time D + 16 (range: 12-38)] and platelets engrafted in 42 patients (70%) [median time D + 17 (range: 12-50)]. Acute GVHD developed in 25 (41.7%) patients [Gr III/IV in 9] and Chronic GVHD in 15 (38.5%). 100-day mortality was 33.8%. With a median follow-up duration of 6.2 months (range: 0.4-50.8 months), the relapse rate, treatment-related mortality (TRM), and estimated 4-year overall survival are 10.0%, 43.3%, and 38.0%, respectively. For the 31 deaths: causes included engraftment failure (n = 7), GVHD (n = 7), persistent disease (n = 1), relapsed disease (n = 5), bacterial sepsis (n = 5), viral pneumonia (n = 1), infection (n = 3), secondary graft failure (n = 2). TRM outcomes have reduced over time with experience. Myeloablative conditioning and haploidentical transplantation by a post-transplant cyclophosphamide approach is feasible in a resource-constrained setting, despite higher rates of GVHD and infection-related mortality.</p>","PeriodicalId":72084,"journal":{"name":"Advances in cell and gene therapy","volume":"4 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2020-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/acg2.106","citationCount":"0","resultStr":"{\"title\":\"Myeloablative haploidentical t-cell replete hematopoietic cell transplantation with post-transplant cyclophosphamide in high-risk hematological malignancies: Bending the learning curve in a middle-income setting\",\"authors\":\"Sanket P. Shah, Vivek S. Radhakrishnan, Ganesh S. Jaishetwar, Reghu K. Sukumaran, Jeevan Kumar, Saurabh J. Bhave, Mita Roychowdhury, Sayak Chaudhuri, Deepak K. Mishra, Reena Nair, Shekhar Krishnan, Mammen Chandy\",\"doi\":\"10.1002/acg2.106\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Haploidentical peripheral blood hematopoietic cell transplantation has become the preferred alternative donor transplant program in most centers in India, owing to its logistic and cost advantages. This is a retrospective analysis of 59 patients with high-risk hematological malignancies who underwent haploidentical transplant in three different centers, using myeloablative conditioning and unmanipulated stem cell graft. GVHD prophylaxis was post-transplant Cyclophosphamide (PTCy D + 3, D + 4) along with Tacrolimus and Mycophenolate Mofetil (D + 5 onwards). The median CD34 cell dose was 5.8 x 10<sup>6</sup> cells/kg. Neutrophils engrafted in 50 (83%) patients [median time D + 16 (range: 12-38)] and platelets engrafted in 42 patients (70%) [median time D + 17 (range: 12-50)]. Acute GVHD developed in 25 (41.7%) patients [Gr III/IV in 9] and Chronic GVHD in 15 (38.5%). 100-day mortality was 33.8%. With a median follow-up duration of 6.2 months (range: 0.4-50.8 months), the relapse rate, treatment-related mortality (TRM), and estimated 4-year overall survival are 10.0%, 43.3%, and 38.0%, respectively. For the 31 deaths: causes included engraftment failure (n = 7), GVHD (n = 7), persistent disease (n = 1), relapsed disease (n = 5), bacterial sepsis (n = 5), viral pneumonia (n = 1), infection (n = 3), secondary graft failure (n = 2). TRM outcomes have reduced over time with experience. Myeloablative conditioning and haploidentical transplantation by a post-transplant cyclophosphamide approach is feasible in a resource-constrained setting, despite higher rates of GVHD and infection-related mortality.</p>\",\"PeriodicalId\":72084,\"journal\":{\"name\":\"Advances in cell and gene therapy\",\"volume\":\"4 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/acg2.106\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in cell and gene therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/acg2.106\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in cell and gene therapy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/acg2.106","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Myeloablative haploidentical t-cell replete hematopoietic cell transplantation with post-transplant cyclophosphamide in high-risk hematological malignancies: Bending the learning curve in a middle-income setting
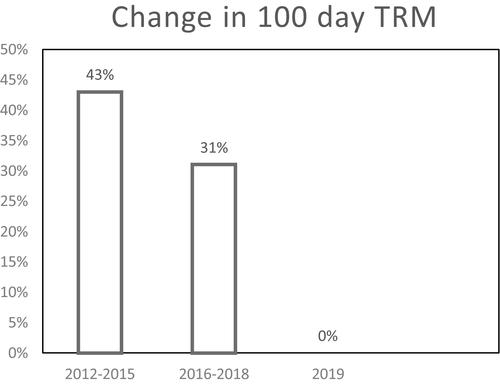
Haploidentical peripheral blood hematopoietic cell transplantation has become the preferred alternative donor transplant program in most centers in India, owing to its logistic and cost advantages. This is a retrospective analysis of 59 patients with high-risk hematological malignancies who underwent haploidentical transplant in three different centers, using myeloablative conditioning and unmanipulated stem cell graft. GVHD prophylaxis was post-transplant Cyclophosphamide (PTCy D + 3, D + 4) along with Tacrolimus and Mycophenolate Mofetil (D + 5 onwards). The median CD34 cell dose was 5.8 x 106 cells/kg. Neutrophils engrafted in 50 (83%) patients [median time D + 16 (range: 12-38)] and platelets engrafted in 42 patients (70%) [median time D + 17 (range: 12-50)]. Acute GVHD developed in 25 (41.7%) patients [Gr III/IV in 9] and Chronic GVHD in 15 (38.5%). 100-day mortality was 33.8%. With a median follow-up duration of 6.2 months (range: 0.4-50.8 months), the relapse rate, treatment-related mortality (TRM), and estimated 4-year overall survival are 10.0%, 43.3%, and 38.0%, respectively. For the 31 deaths: causes included engraftment failure (n = 7), GVHD (n = 7), persistent disease (n = 1), relapsed disease (n = 5), bacterial sepsis (n = 5), viral pneumonia (n = 1), infection (n = 3), secondary graft failure (n = 2). TRM outcomes have reduced over time with experience. Myeloablative conditioning and haploidentical transplantation by a post-transplant cyclophosphamide approach is feasible in a resource-constrained setting, despite higher rates of GVHD and infection-related mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


