İsmail Selçuk, Hüseyin Sicim, Ümmühan Nehir Selçuk, Bülent Barış Güven, Ahmet Turan Yılmaz
{"title":"有症状或动脉瘤性右锁骨下动脉异常修复的三种不同策略","authors":"İsmail Selçuk, Hüseyin Sicim, Ümmühan Nehir Selçuk, Bülent Barış Güven, Ahmet Turan Yılmaz","doi":"10.21470/1678-9741-2021-0439","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In this study, we aimed to present three different methods for symptomatic aberrant right subclavian artery (ARSA) surgery.</p><p><strong>Methods: </strong>We identified 11 consecutive adult patients undergoing symptomatic and/or aneurysmal ARSA repair between January 2016 and December 2020. Symptoms were dysphagia (n=8) and dyspnea + dysphagia (n=3). Six patients had aneurysm formation of the ARSA (mean diameter of 4.2 cm [range 2.8 - 6.3]). All data were analyzed retrospectively.</p><p><strong>Results: </strong>Median age of the patients (7 females/4 males) was 55 years (range 49 - 62). The first four patients (36.4%) underwent hybrid repair using thoracic endovascular aortic repair (TEVAR) and bilateral carotid-subclavian artery bypass (CScBp). Three patients (27.2%) were treated by open ARSA resection/ligation with left mini posterolateral thoracotomy (LMPLT) and right CScBp. And the last four patients (36.4%) underwent ARSA resection/ligation with LMPLT and ascending aorta-right subclavian artery bypass with upper mini sternotomy (UMS). Two of the four patients who underwent TEVAR + bilateral CScBp had continuing dysphagia cause of persistent esophageal compression. Brachial plexus injury developed in one of three patients who underwent LMPLT + right CScBp. Pleural effusion treated with thoracentesis alone was observed in one of four patients who underwent UMS + LMPLT.</p><p><strong>Conclusion: </strong>Among the symptomatic and/or aneurysmal ARSA treatment approaches, surgical and hybrid methods are used. There is still no consensus on how to manage these patients. In our study, we recommend the UMS + LMPLT method, since the risk of complications with anatomical bypass is less, and we have more successful surgical results.</p>","PeriodicalId":54481,"journal":{"name":"Revista Brasileira De Cirurgia Cardiovascular","volume":"37 1","pages":"801-806"},"PeriodicalIF":1.2000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9713644/pdf/","citationCount":"0","resultStr":"{\"title\":\"Three Different Strategies for Repair of Symptomatic or Aneurysmatic Aberrant Right Subclavian Arteries.\",\"authors\":\"İsmail Selçuk, Hüseyin Sicim, Ümmühan Nehir Selçuk, Bülent Barış Güven, Ahmet Turan Yılmaz\",\"doi\":\"10.21470/1678-9741-2021-0439\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>In this study, we aimed to present three different methods for symptomatic aberrant right subclavian artery (ARSA) surgery.</p><p><strong>Methods: </strong>We identified 11 consecutive adult patients undergoing symptomatic and/or aneurysmal ARSA repair between January 2016 and December 2020. Symptoms were dysphagia (n=8) and dyspnea + dysphagia (n=3). Six patients had aneurysm formation of the ARSA (mean diameter of 4.2 cm [range 2.8 - 6.3]). All data were analyzed retrospectively.</p><p><strong>Results: </strong>Median age of the patients (7 females/4 males) was 55 years (range 49 - 62). The first four patients (36.4%) underwent hybrid repair using thoracic endovascular aortic repair (TEVAR) and bilateral carotid-subclavian artery bypass (CScBp). Three patients (27.2%) were treated by open ARSA resection/ligation with left mini posterolateral thoracotomy (LMPLT) and right CScBp. And the last four patients (36.4%) underwent ARSA resection/ligation with LMPLT and ascending aorta-right subclavian artery bypass with upper mini sternotomy (UMS). Two of the four patients who underwent TEVAR + bilateral CScBp had continuing dysphagia cause of persistent esophageal compression. Brachial plexus injury developed in one of three patients who underwent LMPLT + right CScBp. Pleural effusion treated with thoracentesis alone was observed in one of four patients who underwent UMS + LMPLT.</p><p><strong>Conclusion: </strong>Among the symptomatic and/or aneurysmal ARSA treatment approaches, surgical and hybrid methods are used. There is still no consensus on how to manage these patients. In our study, we recommend the UMS + LMPLT method, since the risk of complications with anatomical bypass is less, and we have more successful surgical results.</p>\",\"PeriodicalId\":54481,\"journal\":{\"name\":\"Revista Brasileira De Cirurgia Cardiovascular\",\"volume\":\"37 1\",\"pages\":\"801-806\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9713644/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Revista Brasileira De Cirurgia Cardiovascular\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21470/1678-9741-2021-0439\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Brasileira De Cirurgia Cardiovascular","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21470/1678-9741-2021-0439","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Three Different Strategies for Repair of Symptomatic or Aneurysmatic Aberrant Right Subclavian Arteries.
Introduction: In this study, we aimed to present three different methods for symptomatic aberrant right subclavian artery (ARSA) surgery.
Methods: We identified 11 consecutive adult patients undergoing symptomatic and/or aneurysmal ARSA repair between January 2016 and December 2020. Symptoms were dysphagia (n=8) and dyspnea + dysphagia (n=3). Six patients had aneurysm formation of the ARSA (mean diameter of 4.2 cm [range 2.8 - 6.3]). All data were analyzed retrospectively.
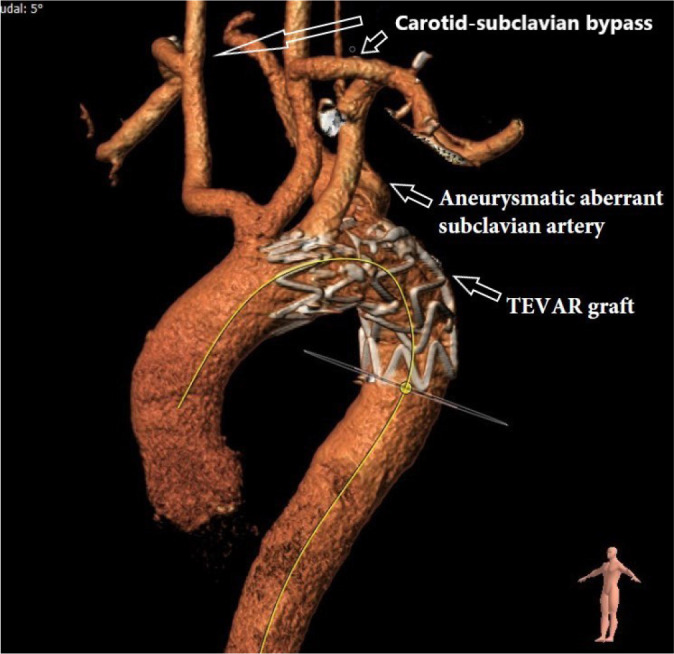
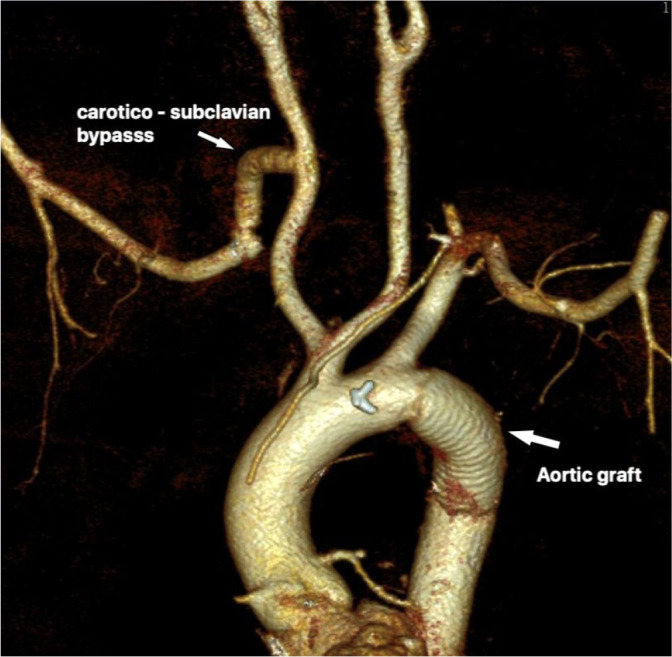
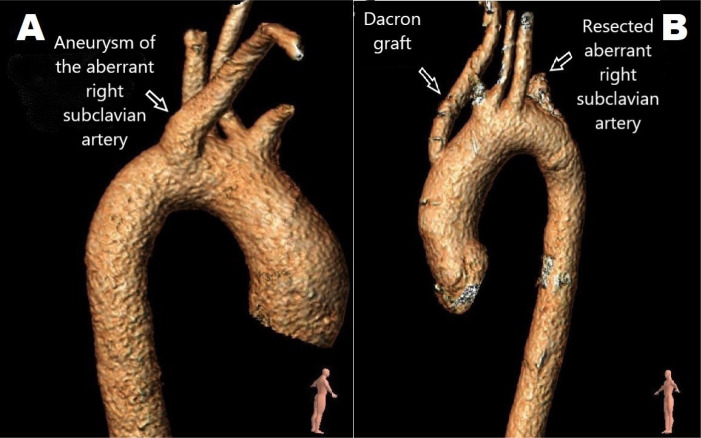
Results: Median age of the patients (7 females/4 males) was 55 years (range 49 - 62). The first four patients (36.4%) underwent hybrid repair using thoracic endovascular aortic repair (TEVAR) and bilateral carotid-subclavian artery bypass (CScBp). Three patients (27.2%) were treated by open ARSA resection/ligation with left mini posterolateral thoracotomy (LMPLT) and right CScBp. And the last four patients (36.4%) underwent ARSA resection/ligation with LMPLT and ascending aorta-right subclavian artery bypass with upper mini sternotomy (UMS). Two of the four patients who underwent TEVAR + bilateral CScBp had continuing dysphagia cause of persistent esophageal compression. Brachial plexus injury developed in one of three patients who underwent LMPLT + right CScBp. Pleural effusion treated with thoracentesis alone was observed in one of four patients who underwent UMS + LMPLT.
Conclusion: Among the symptomatic and/or aneurysmal ARSA treatment approaches, surgical and hybrid methods are used. There is still no consensus on how to manage these patients. In our study, we recommend the UMS + LMPLT method, since the risk of complications with anatomical bypass is less, and we have more successful surgical results.
期刊介绍:
Brazilian Journal of Cardiovascular Surgery (BJCVS) is the official journal of the Brazilian Society of Cardiovascular Surgery (SBCCV). BJCVS is a bimonthly, peer-reviewed scientific journal, with regular circulation since 1986.
BJCVS aims to record the scientific and innovation production in cardiovascular surgery and promote study, improvement and professional updating in the specialty. It has significant impact on cardiovascular surgery practice and related areas.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


