{"title":"剖宫产合并胎盘增生的危险因素及妊娠结局","authors":"Yingyu Liang, Lizi Zhang, Shilei Bi, Jingsi Chen, Shanshan Zeng, Lijun Huang, Yulian Li, Minshan Huang, Hu Tan, Jinping Jia, Suiwen Wen, Zhijian Wang, Yinli Cao, Shaoshuai Wang, Xiaoyan Xu, Ling Feng, Xianlan Zhao, Yangyu Zhao, Qiying Zhu, Hongbo Qi, Lanzhen Zhang, Hongtian Li, Lili Du, Dunjin Chen","doi":"10.1097/FM9.0000000000000142","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To explore the risk factors and pregnancy outcomes in women with a history of cesarean section complicated by placenta accreta (PA).</p><p><strong>Methods: </strong>This case-control study included clinical data from singleton mothers with a history of cesarean section in 11 public tertiary hospitals in seven provinces of China between January 2017 and December 2017. According to the intraoperative findings after delivery, the study population was divided into PA and non-PA groups. We compared the pregnancy outcomes between the two groups, used multivariate logistic regression to analyze the risk factors for placental accreta.</p><p><strong>Results: </strong>For this study we included 11,074 pregnant women with a history of cesarean section; and of these, 869 cases were in the PA group and 10,205 cases were in the non-PA group. Compared with the non-PA group, the probability of postpartum hemorrhage (236/10,205, 2.31% <i>vs</i>. 283/869, 32.57%), severe postpartum hemorrhage (89/10,205, 0.87% <i>vs</i>. 186/869, 21.75%), diffuse intravascular coagulation (3/10,205, 0.03% <i>vs</i>. 4/869, 0.46%), puerperal infection (33/10,205, 0.32% <i>vs</i>. 12/869, 1.38%), intraoperative bladder injury (1/10,205, 0.01% <i>vs</i>. 16/869, 1.84%), hysterectomy (130/10,205, 1.27% <i>vs</i>. 59/869, 6.79%), and blood transfusion (328/10,205,3.21% <i>vs</i>. 231/869,26.58%) was significantly increased in the PA group (<i>P</i> < 0.05). At the same time, the neonatal birth weight (3250.00 (2950.00-3520.00) g <i>vs</i>. 2920.00 (2530.00-3250.00) g), the probability of neonatal comorbidities (245/10,205, 2.40% <i>vs</i>. 61/869, 7.02%), and the rate of neonatal intensive care unit admission (817/10,205, 8.01% <i>vs</i>. 210/869, 24.17%) also increased significantly (<i>P</i> < 0.05). Weight (odds ratio (<i>OR</i>) = 1.03, 95% confidence interval (<i>CI</i>): 1.01-1.05)), parity (<i>OR</i> = 1.18, 95%<i>CI</i>: 1.03-1.34), number of miscarriages (<i>OR</i> = 1.31, 95%<i>CI</i>: 1.17-1.47), number of previous cesarean sections (<i>OR</i> = 2.57, 95%<i>CI</i>: 2.02-3.26), history of premature rupture of membrane (<i>OR</i> = 1.61, 95%<i>CI</i>: 1.32-1.96), previous cesarean-section transverse incisions (<i>OR</i> = 1.38, 95%<i>CI</i>: 1.12-1.69), history of placenta previa (<i>OR</i> = 2.44,95%<i>CI</i>: 1.50-3.96), and the combination of prenatal hemorrhage (<i>OR</i> = 9.95,95%<i>CI</i>: 8.42-11.75) and placenta previa (<i>OR</i> = 91.74, 95%<i>CI</i>: 74.11-113.56) were all independent risk factors for PA.</p><p><strong>Conclusion: </strong>There was an increased risk of adverse outcomes in pregnancies complicated by PA in women with a history of cesarean section, and this required close clinical attention. Weight before pregnancy, parity, number of miscarriages, number of previous cesarean sections, history of premature rupture of membranes, past transverse incisions in cesarean sections, a history of placenta previa, prenatal hemorrhage, and placenta previa were independent risk factors for pregnancies complicated with PA in women with a history of cesarean section. These independent risk factors showed a high value in predicting the risk for placentab accreta in pregnancies of women with a history of cesarean section.</p>","PeriodicalId":74121,"journal":{"name":"Maternal-fetal medicine (Wolters Kluwer Health, Inc.)","volume":"4 1","pages":"179-185"},"PeriodicalIF":1.7000,"publicationDate":"2022-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094359/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors and Pregnancy Outcome in Women with a History of Cesarean Section Complicated by Placenta Accreta.\",\"authors\":\"Yingyu Liang, Lizi Zhang, Shilei Bi, Jingsi Chen, Shanshan Zeng, Lijun Huang, Yulian Li, Minshan Huang, Hu Tan, Jinping Jia, Suiwen Wen, Zhijian Wang, Yinli Cao, Shaoshuai Wang, Xiaoyan Xu, Ling Feng, Xianlan Zhao, Yangyu Zhao, Qiying Zhu, Hongbo Qi, Lanzhen Zhang, Hongtian Li, Lili Du, Dunjin Chen\",\"doi\":\"10.1097/FM9.0000000000000142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To explore the risk factors and pregnancy outcomes in women with a history of cesarean section complicated by placenta accreta (PA).</p><p><strong>Methods: </strong>This case-control study included clinical data from singleton mothers with a history of cesarean section in 11 public tertiary hospitals in seven provinces of China between January 2017 and December 2017. According to the intraoperative findings after delivery, the study population was divided into PA and non-PA groups. We compared the pregnancy outcomes between the two groups, used multivariate logistic regression to analyze the risk factors for placental accreta.</p><p><strong>Results: </strong>For this study we included 11,074 pregnant women with a history of cesarean section; and of these, 869 cases were in the PA group and 10,205 cases were in the non-PA group. Compared with the non-PA group, the probability of postpartum hemorrhage (236/10,205, 2.31% <i>vs</i>. 283/869, 32.57%), severe postpartum hemorrhage (89/10,205, 0.87% <i>vs</i>. 186/869, 21.75%), diffuse intravascular coagulation (3/10,205, 0.03% <i>vs</i>. 4/869, 0.46%), puerperal infection (33/10,205, 0.32% <i>vs</i>. 12/869, 1.38%), intraoperative bladder injury (1/10,205, 0.01% <i>vs</i>. 16/869, 1.84%), hysterectomy (130/10,205, 1.27% <i>vs</i>. 59/869, 6.79%), and blood transfusion (328/10,205,3.21% <i>vs</i>. 231/869,26.58%) was significantly increased in the PA group (<i>P</i> < 0.05). At the same time, the neonatal birth weight (3250.00 (2950.00-3520.00) g <i>vs</i>. 2920.00 (2530.00-3250.00) g), the probability of neonatal comorbidities (245/10,205, 2.40% <i>vs</i>. 61/869, 7.02%), and the rate of neonatal intensive care unit admission (817/10,205, 8.01% <i>vs</i>. 210/869, 24.17%) also increased significantly (<i>P</i> < 0.05). Weight (odds ratio (<i>OR</i>) = 1.03, 95% confidence interval (<i>CI</i>): 1.01-1.05)), parity (<i>OR</i> = 1.18, 95%<i>CI</i>: 1.03-1.34), number of miscarriages (<i>OR</i> = 1.31, 95%<i>CI</i>: 1.17-1.47), number of previous cesarean sections (<i>OR</i> = 2.57, 95%<i>CI</i>: 2.02-3.26), history of premature rupture of membrane (<i>OR</i> = 1.61, 95%<i>CI</i>: 1.32-1.96), previous cesarean-section transverse incisions (<i>OR</i> = 1.38, 95%<i>CI</i>: 1.12-1.69), history of placenta previa (<i>OR</i> = 2.44,95%<i>CI</i>: 1.50-3.96), and the combination of prenatal hemorrhage (<i>OR</i> = 9.95,95%<i>CI</i>: 8.42-11.75) and placenta previa (<i>OR</i> = 91.74, 95%<i>CI</i>: 74.11-113.56) were all independent risk factors for PA.</p><p><strong>Conclusion: </strong>There was an increased risk of adverse outcomes in pregnancies complicated by PA in women with a history of cesarean section, and this required close clinical attention. Weight before pregnancy, parity, number of miscarriages, number of previous cesarean sections, history of premature rupture of membranes, past transverse incisions in cesarean sections, a history of placenta previa, prenatal hemorrhage, and placenta previa were independent risk factors for pregnancies complicated with PA in women with a history of cesarean section. These independent risk factors showed a high value in predicting the risk for placentab accreta in pregnancies of women with a history of cesarean section.</p>\",\"PeriodicalId\":74121,\"journal\":{\"name\":\"Maternal-fetal medicine (Wolters Kluwer Health, Inc.)\",\"volume\":\"4 1\",\"pages\":\"179-185\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094359/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Maternal-fetal medicine (Wolters Kluwer Health, Inc.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/FM9.0000000000000142\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maternal-fetal medicine (Wolters Kluwer Health, Inc.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/FM9.0000000000000142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Risk Factors and Pregnancy Outcome in Women with a History of Cesarean Section Complicated by Placenta Accreta.
Objective: To explore the risk factors and pregnancy outcomes in women with a history of cesarean section complicated by placenta accreta (PA).
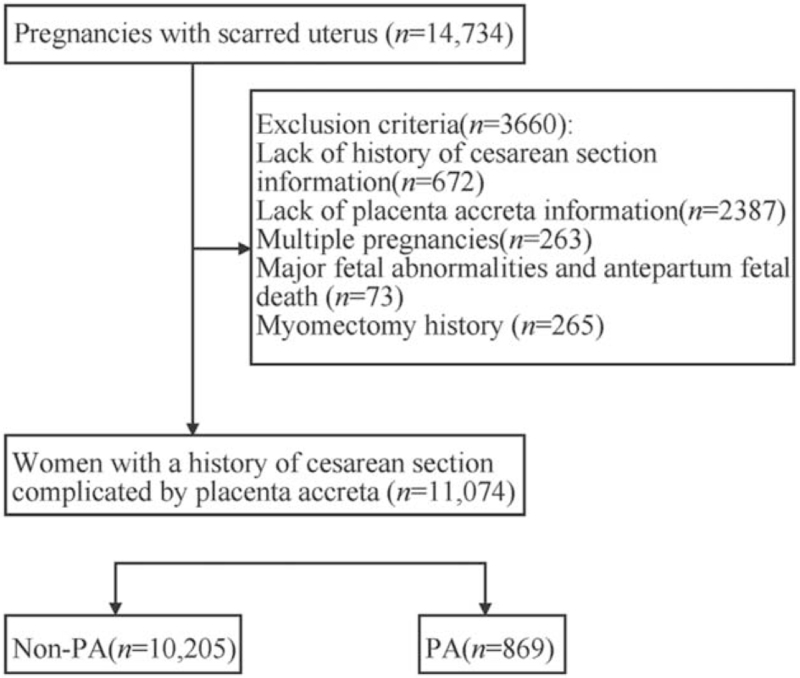
Methods: This case-control study included clinical data from singleton mothers with a history of cesarean section in 11 public tertiary hospitals in seven provinces of China between January 2017 and December 2017. According to the intraoperative findings after delivery, the study population was divided into PA and non-PA groups. We compared the pregnancy outcomes between the two groups, used multivariate logistic regression to analyze the risk factors for placental accreta.
Results: For this study we included 11,074 pregnant women with a history of cesarean section; and of these, 869 cases were in the PA group and 10,205 cases were in the non-PA group. Compared with the non-PA group, the probability of postpartum hemorrhage (236/10,205, 2.31% vs. 283/869, 32.57%), severe postpartum hemorrhage (89/10,205, 0.87% vs. 186/869, 21.75%), diffuse intravascular coagulation (3/10,205, 0.03% vs. 4/869, 0.46%), puerperal infection (33/10,205, 0.32% vs. 12/869, 1.38%), intraoperative bladder injury (1/10,205, 0.01% vs. 16/869, 1.84%), hysterectomy (130/10,205, 1.27% vs. 59/869, 6.79%), and blood transfusion (328/10,205,3.21% vs. 231/869,26.58%) was significantly increased in the PA group (P < 0.05). At the same time, the neonatal birth weight (3250.00 (2950.00-3520.00) g vs. 2920.00 (2530.00-3250.00) g), the probability of neonatal comorbidities (245/10,205, 2.40% vs. 61/869, 7.02%), and the rate of neonatal intensive care unit admission (817/10,205, 8.01% vs. 210/869, 24.17%) also increased significantly (P < 0.05). Weight (odds ratio (OR) = 1.03, 95% confidence interval (CI): 1.01-1.05)), parity (OR = 1.18, 95%CI: 1.03-1.34), number of miscarriages (OR = 1.31, 95%CI: 1.17-1.47), number of previous cesarean sections (OR = 2.57, 95%CI: 2.02-3.26), history of premature rupture of membrane (OR = 1.61, 95%CI: 1.32-1.96), previous cesarean-section transverse incisions (OR = 1.38, 95%CI: 1.12-1.69), history of placenta previa (OR = 2.44,95%CI: 1.50-3.96), and the combination of prenatal hemorrhage (OR = 9.95,95%CI: 8.42-11.75) and placenta previa (OR = 91.74, 95%CI: 74.11-113.56) were all independent risk factors for PA.
Conclusion: There was an increased risk of adverse outcomes in pregnancies complicated by PA in women with a history of cesarean section, and this required close clinical attention. Weight before pregnancy, parity, number of miscarriages, number of previous cesarean sections, history of premature rupture of membranes, past transverse incisions in cesarean sections, a history of placenta previa, prenatal hemorrhage, and placenta previa were independent risk factors for pregnancies complicated with PA in women with a history of cesarean section. These independent risk factors showed a high value in predicting the risk for placentab accreta in pregnancies of women with a history of cesarean section.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


