{"title":"出血的十二指肠病变","authors":"Jhih-Jie Lin, Ming-Jen Chen","doi":"10.1002/aid2.13334","DOIUrl":null,"url":null,"abstract":"<p>A 40-year-old man with no known underlying diseases developed epigastric pain and passed tarry stools for 2 weeks. There was no noted coffee-ground vomitus. Upon arriving at the hospital, he had a hemoglobin level of 9 mg/dL. Esophagogastroduodenoscopy revealed oozing of the duodenal mucosa (Figure 1) The patient underwent blood transfusion with six units of packed red blood cells. Another episode of severe diarrhea with tarry stools and hemodynamic instability occurred after admission. However, no definite extravasation was detected on computed tomography angiography. On repeated esophagogastroduodenoscopy, the previously identified duodenal lesion kept oozing.</p><p>The oozing duodenal mucosa on the opposite side of superior duodenal angle, detected on repeated esophagogastroduodenoscopy, was classified as a Dieulafoy's lesion. Dieulafoy's lesion is a small mucosal erosion into a caliber-persistent and abnormally large submucosal artery. The lesion most commonly affects elderly men, and is typically located in the proximal stomach.<span><sup>1</sup></span></p><p>For the uncommon bleeder with no easily defined feeding vessels, endoscopic band ligation (EBL) was performed using the Multiple Band Ligator (Boston Scientific, The Speedband Superview Super 7, Boston, USA) (Figure 2A) to suction the bleeding target lesion into the cap, occupying the endoscopic view. The rubber band was placed around the bleeding site (Figure 2B). Twenty-seven days after the patient's discharge, repeat esophagogastroduodenoscopy showed a healing scar (Figure 2C).</p><p>Dieulafoy's lesions cause 2% of gastrointestinal hemorrhages, and only 15% of cases involved the duodenum.<span><sup>1</sup></span> For Dieulafoy's lesions, there is no definite consensus on the treatment and the options are dependent on the site of the lesion and available expertise. Several endoscopic techniques have been developed. Some studies have suggested that endoscopic mechanical hemostatic methods were more effective in achieving hemostasis than injection or thermal treatment.<span><sup>2</sup></span> EBL for Dieulafoy's lesions has gained increasing acceptance than hemoclipping because of favorable clinical outcome.<span><sup>3, 4</sup></span> Hemoclipping is sometimes not easy to apply in duodenum when the angle of approach is tangential or when the location has no space to deploy the clip. Delayed bleeding of a residual vessel within a necrotic ulcer is problematic. In one study, about 3% of patients experienced delayed bleeding at the previous EBL site after EBL treatment.<span><sup>5</sup></span></p><p>The authors declare no conflict of interest.</p><p>The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"10 3","pages":"195-196"},"PeriodicalIF":0.3000,"publicationDate":"2022-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13334","citationCount":"0","resultStr":"{\"title\":\"A bleeding duodenal lesion\",\"authors\":\"Jhih-Jie Lin, Ming-Jen Chen\",\"doi\":\"10.1002/aid2.13334\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 40-year-old man with no known underlying diseases developed epigastric pain and passed tarry stools for 2 weeks. There was no noted coffee-ground vomitus. Upon arriving at the hospital, he had a hemoglobin level of 9 mg/dL. Esophagogastroduodenoscopy revealed oozing of the duodenal mucosa (Figure 1) The patient underwent blood transfusion with six units of packed red blood cells. Another episode of severe diarrhea with tarry stools and hemodynamic instability occurred after admission. However, no definite extravasation was detected on computed tomography angiography. On repeated esophagogastroduodenoscopy, the previously identified duodenal lesion kept oozing.</p><p>The oozing duodenal mucosa on the opposite side of superior duodenal angle, detected on repeated esophagogastroduodenoscopy, was classified as a Dieulafoy's lesion. Dieulafoy's lesion is a small mucosal erosion into a caliber-persistent and abnormally large submucosal artery. The lesion most commonly affects elderly men, and is typically located in the proximal stomach.<span><sup>1</sup></span></p><p>For the uncommon bleeder with no easily defined feeding vessels, endoscopic band ligation (EBL) was performed using the Multiple Band Ligator (Boston Scientific, The Speedband Superview Super 7, Boston, USA) (Figure 2A) to suction the bleeding target lesion into the cap, occupying the endoscopic view. The rubber band was placed around the bleeding site (Figure 2B). Twenty-seven days after the patient's discharge, repeat esophagogastroduodenoscopy showed a healing scar (Figure 2C).</p><p>Dieulafoy's lesions cause 2% of gastrointestinal hemorrhages, and only 15% of cases involved the duodenum.<span><sup>1</sup></span> For Dieulafoy's lesions, there is no definite consensus on the treatment and the options are dependent on the site of the lesion and available expertise. Several endoscopic techniques have been developed. Some studies have suggested that endoscopic mechanical hemostatic methods were more effective in achieving hemostasis than injection or thermal treatment.<span><sup>2</sup></span> EBL for Dieulafoy's lesions has gained increasing acceptance than hemoclipping because of favorable clinical outcome.<span><sup>3, 4</sup></span> Hemoclipping is sometimes not easy to apply in duodenum when the angle of approach is tangential or when the location has no space to deploy the clip. Delayed bleeding of a residual vessel within a necrotic ulcer is problematic. In one study, about 3% of patients experienced delayed bleeding at the previous EBL site after EBL treatment.<span><sup>5</sup></span></p><p>The authors declare no conflict of interest.</p><p>The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"10 3\",\"pages\":\"195-196\"},\"PeriodicalIF\":0.3000,\"publicationDate\":\"2022-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13334\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13334\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13334","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
一名40岁男性,无已知基础疾病,出现胃脘痛并排便柏油2周。没有明显的咖啡渣呕吐物。到达医院时,他的血红蛋白水平为9毫克/分升。食管胃十二指肠镜检查显示十二指肠黏膜渗出(图1)。患者接受了6单位填充红细胞输血。入院后再次发生严重腹泻伴柏油便和血流动力学不稳定。然而,计算机断层血管造影未发现明确的外渗。在反复的食管胃十二指肠镜检查中,先前发现的十二指肠病变继续渗出。反复食管胃十二指肠镜检查发现十二指肠上角对侧十二指肠黏膜渗液,为diulafoy病变。Dieulafoy的病变是一个小的粘膜糜烂,进入一个直径持续的和异常大的粘膜下动脉。这种病变最常见于老年男性,通常位于胃近端。对于不容易确定供血血管的罕见出血患者,使用多波段结扎器(Boston Scientific, the Speedband Superview Super 7, Boston, USA)(图2A)进行内镜波段结扎(EBL),将出血目标病灶吸入帽内,占据内镜视野。在出血部位周围放置橡皮筋(图2B)。出院后27天,重复食管胃十二指肠镜检查显示瘢痕愈合(图2C)。diulafoy病变引起2%的胃肠道出血,只有15%的病例累及十二指肠。对于diulafoy的病变,治疗没有明确的共识,选择取决于病变的部位和现有的专业知识。已经开发了几种内窥镜技术。一些研究表明,内镜下机械止血方法比注射或热治疗更有效。由于较好的临床效果,EBL治疗Dieulafoy病变已获得越来越多的认可。当入路角度与十二指肠相切或位置没有空间部署夹血钳时,夹血钳有时不容易应用于十二指肠。坏死血管内残余血管的延迟出血
A 40-year-old man with no known underlying diseases developed epigastric pain and passed tarry stools for 2 weeks. There was no noted coffee-ground vomitus. Upon arriving at the hospital, he had a hemoglobin level of 9 mg/dL. Esophagogastroduodenoscopy revealed oozing of the duodenal mucosa (Figure 1) The patient underwent blood transfusion with six units of packed red blood cells. Another episode of severe diarrhea with tarry stools and hemodynamic instability occurred after admission. However, no definite extravasation was detected on computed tomography angiography. On repeated esophagogastroduodenoscopy, the previously identified duodenal lesion kept oozing.
The oozing duodenal mucosa on the opposite side of superior duodenal angle, detected on repeated esophagogastroduodenoscopy, was classified as a Dieulafoy's lesion. Dieulafoy's lesion is a small mucosal erosion into a caliber-persistent and abnormally large submucosal artery. The lesion most commonly affects elderly men, and is typically located in the proximal stomach.1
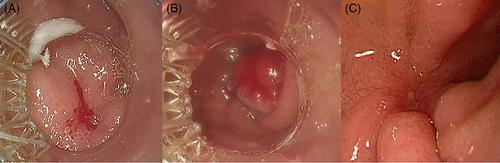
For the uncommon bleeder with no easily defined feeding vessels, endoscopic band ligation (EBL) was performed using the Multiple Band Ligator (Boston Scientific, The Speedband Superview Super 7, Boston, USA) (Figure 2A) to suction the bleeding target lesion into the cap, occupying the endoscopic view. The rubber band was placed around the bleeding site (Figure 2B). Twenty-seven days after the patient's discharge, repeat esophagogastroduodenoscopy showed a healing scar (Figure 2C).
Dieulafoy's lesions cause 2% of gastrointestinal hemorrhages, and only 15% of cases involved the duodenum.1 For Dieulafoy's lesions, there is no definite consensus on the treatment and the options are dependent on the site of the lesion and available expertise. Several endoscopic techniques have been developed. Some studies have suggested that endoscopic mechanical hemostatic methods were more effective in achieving hemostasis than injection or thermal treatment.2 EBL for Dieulafoy's lesions has gained increasing acceptance than hemoclipping because of favorable clinical outcome.3, 4 Hemoclipping is sometimes not easy to apply in duodenum when the angle of approach is tangential or when the location has no space to deploy the clip. Delayed bleeding of a residual vessel within a necrotic ulcer is problematic. In one study, about 3% of patients experienced delayed bleeding at the previous EBL site after EBL treatment.5
The authors declare no conflict of interest.
The study participant provided informed consent, and the study design was approved by the appropriate ethics review board.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


