{"title":"正常互补性荨麻疹血管炎伴喉部和肠道水肿","authors":"Daisuke Kawakami MD, Yoshiko Oda MD, PhD, Yumi Oka MD, Anri Morita MD, Keiko Kuroda MD, Yoji Hirai MD, PhD, Chikako Nishigori MD, PhD, Atsushi Fukunaga MD, PhD","doi":"10.1002/cia2.12312","DOIUrl":null,"url":null,"abstract":"<p>An 81-year-old Japanese man presented with a history of recurrent eyelid swelling and purpura on the face, neck, and limbs. Because the initial clinical presentation was angioedema alone, the patient was treated with an H1-receptor antagonist and tranexamic acid as for an idiopathic angioedema. The patient also experienced dyspnea simultaneously with edema on the face and limbs and was thus taken to the emergency room, where laryngeal edema was confirmed on laryngeal fiber. A good response to hydrocortisone injection was observed in the patient. ACE inhibitors were never prescribed for the patient, and there was no family history of angioedema. Laboratory data indicated normocomplementemia, and skin biopsies revealed leukocytoclastic vasculitis. Therefore, the patient was diagnosed with NUV. Following hospitalization, the patient experienced appetite loss and the CRP level increased, presenting with thickening and stranding around colon tissues on abdominal CT. These symptoms responded well to prednisone treatment. Given that the initial clinical manifestation of the current case was mainly angioedema, physicians should consider that angioedema may in rare cases be diagnostic for UV.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 5","pages":"172-174"},"PeriodicalIF":0.9000,"publicationDate":"2023-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12312","citationCount":"0","resultStr":"{\"title\":\"Normocomplementemic urticarial vasculitis with laryngeal and intestinal tract edema\",\"authors\":\"Daisuke Kawakami MD, Yoshiko Oda MD, PhD, Yumi Oka MD, Anri Morita MD, Keiko Kuroda MD, Yoji Hirai MD, PhD, Chikako Nishigori MD, PhD, Atsushi Fukunaga MD, PhD\",\"doi\":\"10.1002/cia2.12312\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>An 81-year-old Japanese man presented with a history of recurrent eyelid swelling and purpura on the face, neck, and limbs. Because the initial clinical presentation was angioedema alone, the patient was treated with an H1-receptor antagonist and tranexamic acid as for an idiopathic angioedema. The patient also experienced dyspnea simultaneously with edema on the face and limbs and was thus taken to the emergency room, where laryngeal edema was confirmed on laryngeal fiber. A good response to hydrocortisone injection was observed in the patient. ACE inhibitors were never prescribed for the patient, and there was no family history of angioedema. Laboratory data indicated normocomplementemia, and skin biopsies revealed leukocytoclastic vasculitis. Therefore, the patient was diagnosed with NUV. Following hospitalization, the patient experienced appetite loss and the CRP level increased, presenting with thickening and stranding around colon tissues on abdominal CT. These symptoms responded well to prednisone treatment. Given that the initial clinical manifestation of the current case was mainly angioedema, physicians should consider that angioedema may in rare cases be diagnostic for UV.</p>\",\"PeriodicalId\":15543,\"journal\":{\"name\":\"Journal of Cutaneous Immunology and Allergy\",\"volume\":\"6 5\",\"pages\":\"172-174\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-08-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12312\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cutaneous Immunology and Allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12312\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12312","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
Normocomplementemic urticarial vasculitis with laryngeal and intestinal tract edema
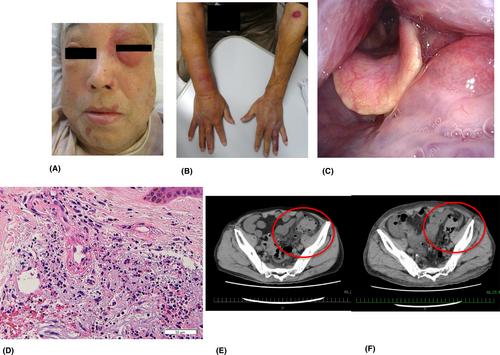
An 81-year-old Japanese man presented with a history of recurrent eyelid swelling and purpura on the face, neck, and limbs. Because the initial clinical presentation was angioedema alone, the patient was treated with an H1-receptor antagonist and tranexamic acid as for an idiopathic angioedema. The patient also experienced dyspnea simultaneously with edema on the face and limbs and was thus taken to the emergency room, where laryngeal edema was confirmed on laryngeal fiber. A good response to hydrocortisone injection was observed in the patient. ACE inhibitors were never prescribed for the patient, and there was no family history of angioedema. Laboratory data indicated normocomplementemia, and skin biopsies revealed leukocytoclastic vasculitis. Therefore, the patient was diagnosed with NUV. Following hospitalization, the patient experienced appetite loss and the CRP level increased, presenting with thickening and stranding around colon tissues on abdominal CT. These symptoms responded well to prednisone treatment. Given that the initial clinical manifestation of the current case was mainly angioedema, physicians should consider that angioedema may in rare cases be diagnostic for UV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


