{"title":"接种新冠疫苗后的非典型皮下起泡病","authors":"Noureddine Litaiem MD, Azza Ghannem MD, Amal Chabbouh MD, Soumaya Rammeh MD, Maryam Sellami MD, Faten Zeglaoui MD","doi":"10.1002/cia2.12308","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Cutaneous bullous eruptions triggered after COVID-19 vaccination have been reported.<span><sup>1</sup></span> However, a few cases of these blistering disorders have shown an atypical immunological profile. We present a distinctive case of an acquired bullous eruption in a 79-year-old patient appearing days after COVID-19 booster vaccination shot.</p><p>A 79-year-old female patient, with no past medical history or regular drug intake presented with a new onset of pruritic cutaneous blisters appearing 1 week after COVID-19 vaccination booster shot. She received two shots of Sinovac-CoronaVac vaccine, and a third shot using Pfizer-BioNTech Vaccine. Physical examination revealed tense and hemorrhagic blisters on normal-appearing, purpuric or erythematous skin (Figure 1A–C). Lesions were symmetrically distributed on the upper and lower limbs and sparing oral and genital mucosa. Nikolsky's sign was positive on purpuric skin. Skin biopsies were repeatedly performed showing similar results (Figure 1D,E). Histopathological examination revealed subepidermal blisters with numerous necrotic keratinocytes and vacuolar degeneration of basal epidermal cells associated with a lymphocytic inflammatory infiltrate of the dermis with no eosinophils. Direct immunofluorescence examination showed marked intradermal deposits of IgG, IgM, IgA, C3, and C1q within necrotic keratinocytes of the epidermis (Figure 1F). Indirect immunofluorescence and ELISA Testing for anti-desmoglein1, anti-desmoglein3, anti-BP180, and anti-BP230 were negative. A complete blood count results including eosinophil count were within normal range. Lesions kept progressing for 8 months. The patient denied any drug intake or infection preceding disease onset or relapse. The diagnosis of subepidermal blistering disease triggered by COVID-19 vaccination was made. The patient received clobetasol ointment leading to temporary control of the disease. However, blisters relapsed days after treatment discontinuation and were similarly managed with topical corticosteroids.</p><p>Subepidermal bullous eruptions following vaccination represent an immune-mediated event related to nonspecific off-target immune response.<span><sup>1</sup></span> Bullous pemphigoid is the most frequently reported auto-immune blistering disorder appearing after COVID-19 vaccination.<span><sup>2</sup></span> Pemphigus was less frequently associated with vaccination.<span><sup>3</sup></span> Our patient was remarkable as she had a chronic and relapsing disease that failed to meet the diagnostic criteria of pemphigus, pemphigoid, or any other auto-immune blistering disorder.</p><p>A few cases of Steven-Johnson syndrome/Toxic epidermal necrosis have been reported in response to virotope antigens of the COVID-19 vaccine.<span><sup>4</sup></span> These virotopes are expressed on the keratinocyte surface. This leads to CD8<sup>+</sup> T lymphocyte activation and epidermal cell apoptosis with subepidermal detachment.<span><sup>4</sup></span> Kong et al.<span><sup>5</sup></span> described a case of subepidermal blistering eruption following Moderna vaccine showing marked necrotic keratinocytes. In these cases, DIF and IIF were not performed.</p><p>In our patient, the clinical presentation was not consistent with the diagnosis of Steven-Johnson syndrome/Toxic epidermal necrosis. The negativity of DIF and anti-BP180/BP230 clearly emphasizes the cellular-mediated response.</p><p>Five other cases of subepidermal bullous eruptions following COVID-19 vaccination with atypical clinical or immunopathological features similar to our patient were described (Table 1). Tomayko et al.<span><sup>1</sup></span> reported four cases of subepidermal blistering disorders with negative DIF and serum anti-BP180/anti-BP230 antibodies.</p><p>These findings may arguably raise concern over the possibility of a distinct variant of subepidermal blistering eruption induced by these newly developed mRNA vaccines. However, this association is still debated.<span><sup>6</sup></span> Although a coincidence cannot be excluded, the short delay suggests a close relation between COVID-19 vaccination and this bullous disorder. The autonomization of the disease as a chronic blistering disorder after the removal of the culprit trigger requires longitudinal follow-up.<span><sup>7</sup></span> There are no drawing conclusions about avoidance or possible vaccinations. Our patient refused the new vaccination.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed Consent: The patient provided informed consent for the publication of the images submitted with this article.</p><p>Registry and the Registration No.: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 5","pages":"179-182"},"PeriodicalIF":0.9000,"publicationDate":"2023-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12308","citationCount":"0","resultStr":"{\"title\":\"Atypical subepidermal blistering disease following COVID-19 vaccination\",\"authors\":\"Noureddine Litaiem MD, Azza Ghannem MD, Amal Chabbouh MD, Soumaya Rammeh MD, Maryam Sellami MD, Faten Zeglaoui MD\",\"doi\":\"10.1002/cia2.12308\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor,</p><p>Cutaneous bullous eruptions triggered after COVID-19 vaccination have been reported.<span><sup>1</sup></span> However, a few cases of these blistering disorders have shown an atypical immunological profile. We present a distinctive case of an acquired bullous eruption in a 79-year-old patient appearing days after COVID-19 booster vaccination shot.</p><p>A 79-year-old female patient, with no past medical history or regular drug intake presented with a new onset of pruritic cutaneous blisters appearing 1 week after COVID-19 vaccination booster shot. She received two shots of Sinovac-CoronaVac vaccine, and a third shot using Pfizer-BioNTech Vaccine. Physical examination revealed tense and hemorrhagic blisters on normal-appearing, purpuric or erythematous skin (Figure 1A–C). Lesions were symmetrically distributed on the upper and lower limbs and sparing oral and genital mucosa. Nikolsky's sign was positive on purpuric skin. Skin biopsies were repeatedly performed showing similar results (Figure 1D,E). Histopathological examination revealed subepidermal blisters with numerous necrotic keratinocytes and vacuolar degeneration of basal epidermal cells associated with a lymphocytic inflammatory infiltrate of the dermis with no eosinophils. Direct immunofluorescence examination showed marked intradermal deposits of IgG, IgM, IgA, C3, and C1q within necrotic keratinocytes of the epidermis (Figure 1F). Indirect immunofluorescence and ELISA Testing for anti-desmoglein1, anti-desmoglein3, anti-BP180, and anti-BP230 were negative. A complete blood count results including eosinophil count were within normal range. Lesions kept progressing for 8 months. The patient denied any drug intake or infection preceding disease onset or relapse. The diagnosis of subepidermal blistering disease triggered by COVID-19 vaccination was made. The patient received clobetasol ointment leading to temporary control of the disease. However, blisters relapsed days after treatment discontinuation and were similarly managed with topical corticosteroids.</p><p>Subepidermal bullous eruptions following vaccination represent an immune-mediated event related to nonspecific off-target immune response.<span><sup>1</sup></span> Bullous pemphigoid is the most frequently reported auto-immune blistering disorder appearing after COVID-19 vaccination.<span><sup>2</sup></span> Pemphigus was less frequently associated with vaccination.<span><sup>3</sup></span> Our patient was remarkable as she had a chronic and relapsing disease that failed to meet the diagnostic criteria of pemphigus, pemphigoid, or any other auto-immune blistering disorder.</p><p>A few cases of Steven-Johnson syndrome/Toxic epidermal necrosis have been reported in response to virotope antigens of the COVID-19 vaccine.<span><sup>4</sup></span> These virotopes are expressed on the keratinocyte surface. This leads to CD8<sup>+</sup> T lymphocyte activation and epidermal cell apoptosis with subepidermal detachment.<span><sup>4</sup></span> Kong et al.<span><sup>5</sup></span> described a case of subepidermal blistering eruption following Moderna vaccine showing marked necrotic keratinocytes. In these cases, DIF and IIF were not performed.</p><p>In our patient, the clinical presentation was not consistent with the diagnosis of Steven-Johnson syndrome/Toxic epidermal necrosis. The negativity of DIF and anti-BP180/BP230 clearly emphasizes the cellular-mediated response.</p><p>Five other cases of subepidermal bullous eruptions following COVID-19 vaccination with atypical clinical or immunopathological features similar to our patient were described (Table 1). Tomayko et al.<span><sup>1</sup></span> reported four cases of subepidermal blistering disorders with negative DIF and serum anti-BP180/anti-BP230 antibodies.</p><p>These findings may arguably raise concern over the possibility of a distinct variant of subepidermal blistering eruption induced by these newly developed mRNA vaccines. However, this association is still debated.<span><sup>6</sup></span> Although a coincidence cannot be excluded, the short delay suggests a close relation between COVID-19 vaccination and this bullous disorder. The autonomization of the disease as a chronic blistering disorder after the removal of the culprit trigger requires longitudinal follow-up.<span><sup>7</sup></span> There are no drawing conclusions about avoidance or possible vaccinations. Our patient refused the new vaccination.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed Consent: The patient provided informed consent for the publication of the images submitted with this article.</p><p>Registry and the Registration No.: N/A.</p><p>Animal Studies: N/A.</p>\",\"PeriodicalId\":15543,\"journal\":{\"name\":\"Journal of Cutaneous Immunology and Allergy\",\"volume\":\"6 5\",\"pages\":\"179-182\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-06-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12308\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cutaneous Immunology and Allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12308\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12308","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
Atypical subepidermal blistering disease following COVID-19 vaccination
Dear Editor,
Cutaneous bullous eruptions triggered after COVID-19 vaccination have been reported.1 However, a few cases of these blistering disorders have shown an atypical immunological profile. We present a distinctive case of an acquired bullous eruption in a 79-year-old patient appearing days after COVID-19 booster vaccination shot.
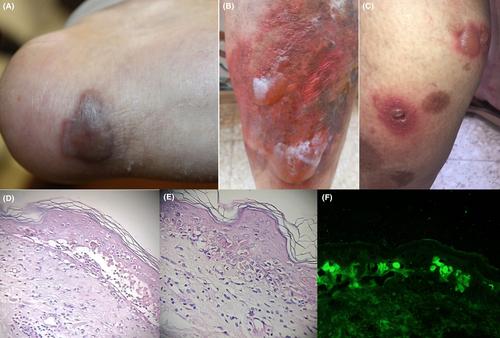
A 79-year-old female patient, with no past medical history or regular drug intake presented with a new onset of pruritic cutaneous blisters appearing 1 week after COVID-19 vaccination booster shot. She received two shots of Sinovac-CoronaVac vaccine, and a third shot using Pfizer-BioNTech Vaccine. Physical examination revealed tense and hemorrhagic blisters on normal-appearing, purpuric or erythematous skin (Figure 1A–C). Lesions were symmetrically distributed on the upper and lower limbs and sparing oral and genital mucosa. Nikolsky's sign was positive on purpuric skin. Skin biopsies were repeatedly performed showing similar results (Figure 1D,E). Histopathological examination revealed subepidermal blisters with numerous necrotic keratinocytes and vacuolar degeneration of basal epidermal cells associated with a lymphocytic inflammatory infiltrate of the dermis with no eosinophils. Direct immunofluorescence examination showed marked intradermal deposits of IgG, IgM, IgA, C3, and C1q within necrotic keratinocytes of the epidermis (Figure 1F). Indirect immunofluorescence and ELISA Testing for anti-desmoglein1, anti-desmoglein3, anti-BP180, and anti-BP230 were negative. A complete blood count results including eosinophil count were within normal range. Lesions kept progressing for 8 months. The patient denied any drug intake or infection preceding disease onset or relapse. The diagnosis of subepidermal blistering disease triggered by COVID-19 vaccination was made. The patient received clobetasol ointment leading to temporary control of the disease. However, blisters relapsed days after treatment discontinuation and were similarly managed with topical corticosteroids.
Subepidermal bullous eruptions following vaccination represent an immune-mediated event related to nonspecific off-target immune response.1 Bullous pemphigoid is the most frequently reported auto-immune blistering disorder appearing after COVID-19 vaccination.2 Pemphigus was less frequently associated with vaccination.3 Our patient was remarkable as she had a chronic and relapsing disease that failed to meet the diagnostic criteria of pemphigus, pemphigoid, or any other auto-immune blistering disorder.
A few cases of Steven-Johnson syndrome/Toxic epidermal necrosis have been reported in response to virotope antigens of the COVID-19 vaccine.4 These virotopes are expressed on the keratinocyte surface. This leads to CD8+ T lymphocyte activation and epidermal cell apoptosis with subepidermal detachment.4 Kong et al.5 described a case of subepidermal blistering eruption following Moderna vaccine showing marked necrotic keratinocytes. In these cases, DIF and IIF were not performed.
In our patient, the clinical presentation was not consistent with the diagnosis of Steven-Johnson syndrome/Toxic epidermal necrosis. The negativity of DIF and anti-BP180/BP230 clearly emphasizes the cellular-mediated response.
Five other cases of subepidermal bullous eruptions following COVID-19 vaccination with atypical clinical or immunopathological features similar to our patient were described (Table 1). Tomayko et al.1 reported four cases of subepidermal blistering disorders with negative DIF and serum anti-BP180/anti-BP230 antibodies.
These findings may arguably raise concern over the possibility of a distinct variant of subepidermal blistering eruption induced by these newly developed mRNA vaccines. However, this association is still debated.6 Although a coincidence cannot be excluded, the short delay suggests a close relation between COVID-19 vaccination and this bullous disorder. The autonomization of the disease as a chronic blistering disorder after the removal of the culprit trigger requires longitudinal follow-up.7 There are no drawing conclusions about avoidance or possible vaccinations. Our patient refused the new vaccination.
The authors declare no conflict of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed Consent: The patient provided informed consent for the publication of the images submitted with this article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


