{"title":"Pudendal神经交叉支配改良尿道成形术治疗前列腺切除术后尿失禁:尸体模拟手术和临床病例报告","authors":"Hisashi Sakuma, Masaki Yazawa, Makoto Hikosaka, Yumiko Uchikawa-Tani, Masayoshi Takayama, Kazuo Kishi","doi":"10.1055/a-1995-1513","DOIUrl":null,"url":null,"abstract":"<p><p>An artificial sphincter implanted in the bulbous urethra to treat severe postprostatectomy urinary incontinence is effective, but embedding-associated complications can occur. We assessed the feasibility, efficacy, and safety of urethral graciloplasty cross-innervated by the pudendal nerve. A simulation surgery on three male fresh cadavers was performed. Both ends of the gracilis muscle were isolated only on its vascular pedicle with proximal end of the obturator nerve severed and transferred to the perineum. We examined whether the gracilis muscle could be wrapped around the bulbous urethra and whether the obturator nerve was long enough to suture with the pudendal nerve. In addition, surgery was performed on a 71-year-old male patient with severe urinary incontinence. The postoperative 12-month outcomes were assessed using a 24-hour pad test and urodynamic study. In all cadaveric simulations, the gracilis muscles could be wrapped around the bulbous urethra in a γ-loop configuration. The length of the obturator nerve was sufficient for neurorrhaphy with the pudendal nerve. In the clinical case, the postoperative course was uneventful. The mean maximum urethral closure pressure and functional profile length increased from 40.7 to 70 cm H <sub>2</sub> O and from 40.1 to 45.3 mm, respectively. Although urinary incontinence was not completely cured, the patient was able to maintain urinary continence at night. Urethral graciloplasty cross-innervated by the pudendal nerve is effective in raising the urethral pressure and reducing urinary incontinence.</p>","PeriodicalId":47543,"journal":{"name":"Archives of Plastic Surgery-APS","volume":"1 1","pages":"578-585"},"PeriodicalIF":1.5000,"publicationDate":"2023-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10736196/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modified Urethral Graciloplasty Cross-Innervated by the Pudendal Nerve for Postprostatectomy Urinary Incontinence: Cadaveric Simulation Surgery and a Clinical Case Report.\",\"authors\":\"Hisashi Sakuma, Masaki Yazawa, Makoto Hikosaka, Yumiko Uchikawa-Tani, Masayoshi Takayama, Kazuo Kishi\",\"doi\":\"10.1055/a-1995-1513\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>An artificial sphincter implanted in the bulbous urethra to treat severe postprostatectomy urinary incontinence is effective, but embedding-associated complications can occur. We assessed the feasibility, efficacy, and safety of urethral graciloplasty cross-innervated by the pudendal nerve. A simulation surgery on three male fresh cadavers was performed. Both ends of the gracilis muscle were isolated only on its vascular pedicle with proximal end of the obturator nerve severed and transferred to the perineum. We examined whether the gracilis muscle could be wrapped around the bulbous urethra and whether the obturator nerve was long enough to suture with the pudendal nerve. In addition, surgery was performed on a 71-year-old male patient with severe urinary incontinence. The postoperative 12-month outcomes were assessed using a 24-hour pad test and urodynamic study. In all cadaveric simulations, the gracilis muscles could be wrapped around the bulbous urethra in a γ-loop configuration. The length of the obturator nerve was sufficient for neurorrhaphy with the pudendal nerve. In the clinical case, the postoperative course was uneventful. The mean maximum urethral closure pressure and functional profile length increased from 40.7 to 70 cm H <sub>2</sub> O and from 40.1 to 45.3 mm, respectively. Although urinary incontinence was not completely cured, the patient was able to maintain urinary continence at night. Urethral graciloplasty cross-innervated by the pudendal nerve is effective in raising the urethral pressure and reducing urinary incontinence.</p>\",\"PeriodicalId\":47543,\"journal\":{\"name\":\"Archives of Plastic Surgery-APS\",\"volume\":\"1 1\",\"pages\":\"578-585\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-10-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10736196/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Plastic Surgery-APS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-1995-1513\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Plastic Surgery-APS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-1995-1513","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Modified Urethral Graciloplasty Cross-Innervated by the Pudendal Nerve for Postprostatectomy Urinary Incontinence: Cadaveric Simulation Surgery and a Clinical Case Report.
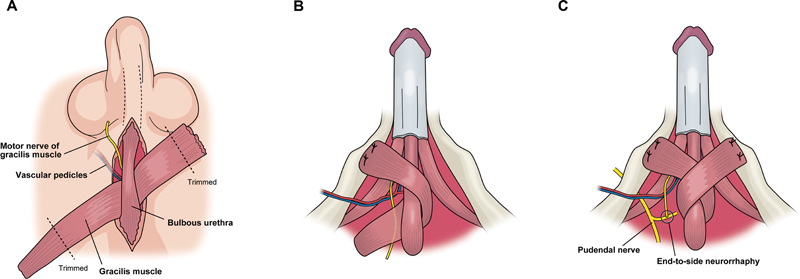
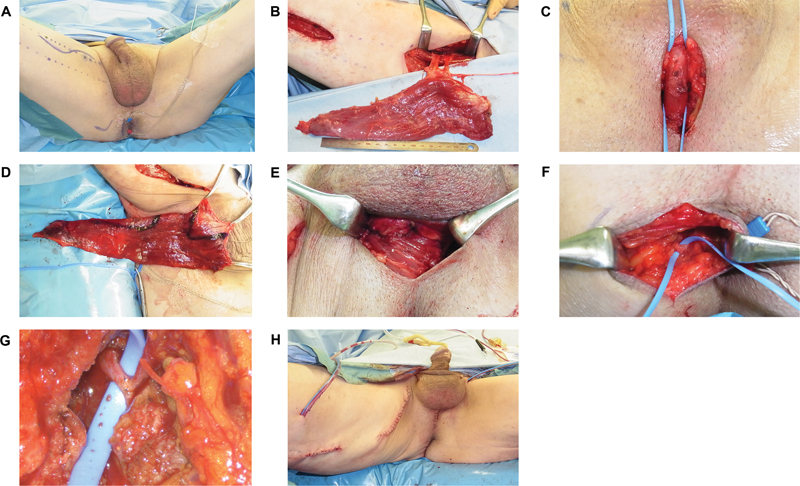
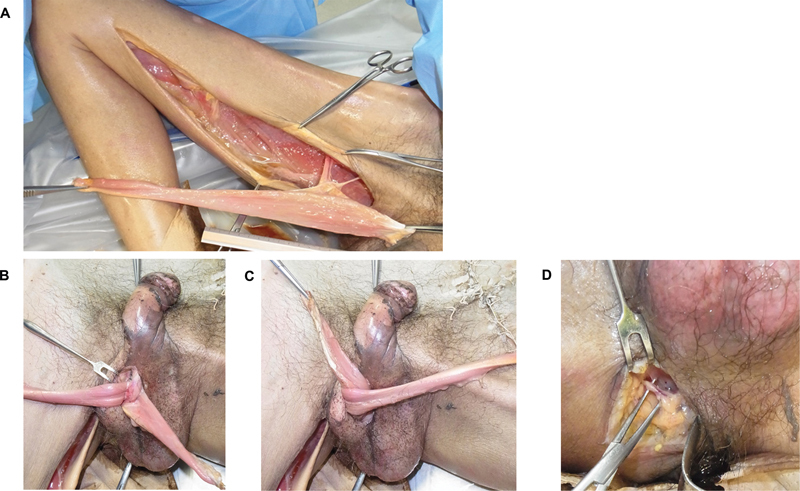
An artificial sphincter implanted in the bulbous urethra to treat severe postprostatectomy urinary incontinence is effective, but embedding-associated complications can occur. We assessed the feasibility, efficacy, and safety of urethral graciloplasty cross-innervated by the pudendal nerve. A simulation surgery on three male fresh cadavers was performed. Both ends of the gracilis muscle were isolated only on its vascular pedicle with proximal end of the obturator nerve severed and transferred to the perineum. We examined whether the gracilis muscle could be wrapped around the bulbous urethra and whether the obturator nerve was long enough to suture with the pudendal nerve. In addition, surgery was performed on a 71-year-old male patient with severe urinary incontinence. The postoperative 12-month outcomes were assessed using a 24-hour pad test and urodynamic study. In all cadaveric simulations, the gracilis muscles could be wrapped around the bulbous urethra in a γ-loop configuration. The length of the obturator nerve was sufficient for neurorrhaphy with the pudendal nerve. In the clinical case, the postoperative course was uneventful. The mean maximum urethral closure pressure and functional profile length increased from 40.7 to 70 cm H 2 O and from 40.1 to 45.3 mm, respectively. Although urinary incontinence was not completely cured, the patient was able to maintain urinary continence at night. Urethral graciloplasty cross-innervated by the pudendal nerve is effective in raising the urethral pressure and reducing urinary incontinence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


