K C Sadik, Devendra Mishra, Monica Juneja, Urmila Jhamb
{"title":"印度一家公立医院小儿难治性癫痫的临床病因简介。","authors":"K C Sadik, Devendra Mishra, Monica Juneja, Urmila Jhamb","doi":"10.14581/jer.19004","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Refractory status epilepticus (RSE) has been infrequently studied in Indian children. This research was conducted to study the clinico-etiological profiles and short-term outcomes of children aged 1 month to 12 years with convulsive RSE, at a public hospital.</p><p><strong>Methods: </strong>The study was conducted between 1st April 2016 and 28th February 2017 after receiving clearance from an Institutional Ethics Committee. All children (aged 1 month to 12 years) who presented to the pediatrics department of a tertiary-care public hospital with convulsive status epilepticus (SE), or who developed SE during their hospital stay, were enrolled. All patients were investigated and managed according to a standard protocol. Outcomes were assessed based on the Glasgow Outcome Scale. Details of children who progressed to RSE were compared to those without RSE.</p><p><strong>Results: </strong>Fifty children (28 males) with CSE were enrolled, of which 20 (40%) progressed to RSE. Central nervous system (CNS) infection was the most common etiology (53% in SE and 55% in RSE, <i>p</i> > 0.05). Non-compliance with anti-epileptic drugs was the second most common etiology. The overall mortality rate was 38%, and although the odds of death in RSE (50%) were higher than in SE (30%), this difference was not statistically significant (<i>p</i> = 0.15). The odds of having a poor outcome was six times higher in children with RSE as compared to those with SE (odds ratio, 6.0; 95% confidence interval, 1.6-22.3; <i>p</i> = 0.005).</p><p><strong>Conclusions: </strong>When managing CNS infections, pediatricians need to be aware of the high risk of developing RSE. In addition, the possibility of RSE should be considered and managed promptly in an intensive-care setting, to reduce the mortality and morbidity of this severe neurological condition.</p>","PeriodicalId":73741,"journal":{"name":"Journal of epilepsy research","volume":"9 1","pages":"36-41"},"PeriodicalIF":0.0000,"publicationDate":"2019-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7d/7e/er-9-1-36.PMC6706643.pdf","citationCount":"8","resultStr":"{\"title\":\"Clinico-Etiological Profile of Pediatric Refractory Status Epilepticus at a Public Hospital in India.\",\"authors\":\"K C Sadik, Devendra Mishra, Monica Juneja, Urmila Jhamb\",\"doi\":\"10.14581/jer.19004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Refractory status epilepticus (RSE) has been infrequently studied in Indian children. This research was conducted to study the clinico-etiological profiles and short-term outcomes of children aged 1 month to 12 years with convulsive RSE, at a public hospital.</p><p><strong>Methods: </strong>The study was conducted between 1st April 2016 and 28th February 2017 after receiving clearance from an Institutional Ethics Committee. All children (aged 1 month to 12 years) who presented to the pediatrics department of a tertiary-care public hospital with convulsive status epilepticus (SE), or who developed SE during their hospital stay, were enrolled. All patients were investigated and managed according to a standard protocol. Outcomes were assessed based on the Glasgow Outcome Scale. Details of children who progressed to RSE were compared to those without RSE.</p><p><strong>Results: </strong>Fifty children (28 males) with CSE were enrolled, of which 20 (40%) progressed to RSE. Central nervous system (CNS) infection was the most common etiology (53% in SE and 55% in RSE, <i>p</i> > 0.05). Non-compliance with anti-epileptic drugs was the second most common etiology. The overall mortality rate was 38%, and although the odds of death in RSE (50%) were higher than in SE (30%), this difference was not statistically significant (<i>p</i> = 0.15). The odds of having a poor outcome was six times higher in children with RSE as compared to those with SE (odds ratio, 6.0; 95% confidence interval, 1.6-22.3; <i>p</i> = 0.005).</p><p><strong>Conclusions: </strong>When managing CNS infections, pediatricians need to be aware of the high risk of developing RSE. In addition, the possibility of RSE should be considered and managed promptly in an intensive-care setting, to reduce the mortality and morbidity of this severe neurological condition.</p>\",\"PeriodicalId\":73741,\"journal\":{\"name\":\"Journal of epilepsy research\",\"volume\":\"9 1\",\"pages\":\"36-41\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7d/7e/er-9-1-36.PMC6706643.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of epilepsy research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14581/jer.19004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of epilepsy research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14581/jer.19004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Clinico-Etiological Profile of Pediatric Refractory Status Epilepticus at a Public Hospital in India.
Background and purpose: Refractory status epilepticus (RSE) has been infrequently studied in Indian children. This research was conducted to study the clinico-etiological profiles and short-term outcomes of children aged 1 month to 12 years with convulsive RSE, at a public hospital.
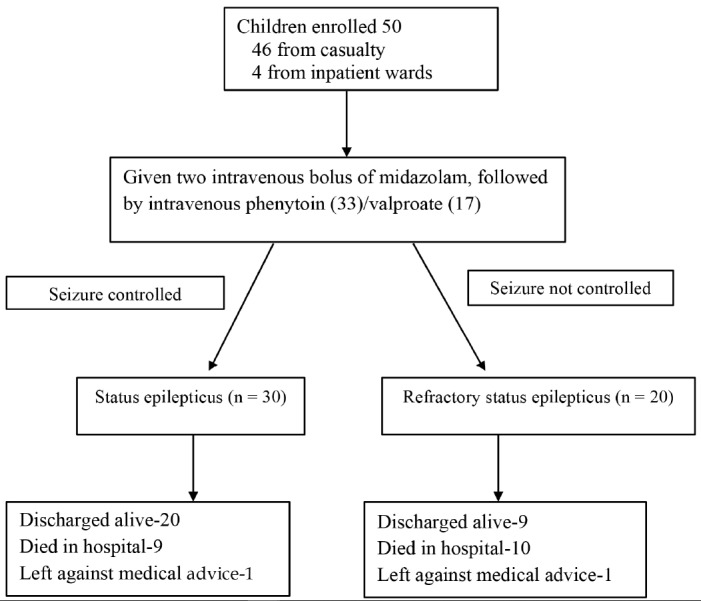
Methods: The study was conducted between 1st April 2016 and 28th February 2017 after receiving clearance from an Institutional Ethics Committee. All children (aged 1 month to 12 years) who presented to the pediatrics department of a tertiary-care public hospital with convulsive status epilepticus (SE), or who developed SE during their hospital stay, were enrolled. All patients were investigated and managed according to a standard protocol. Outcomes were assessed based on the Glasgow Outcome Scale. Details of children who progressed to RSE were compared to those without RSE.
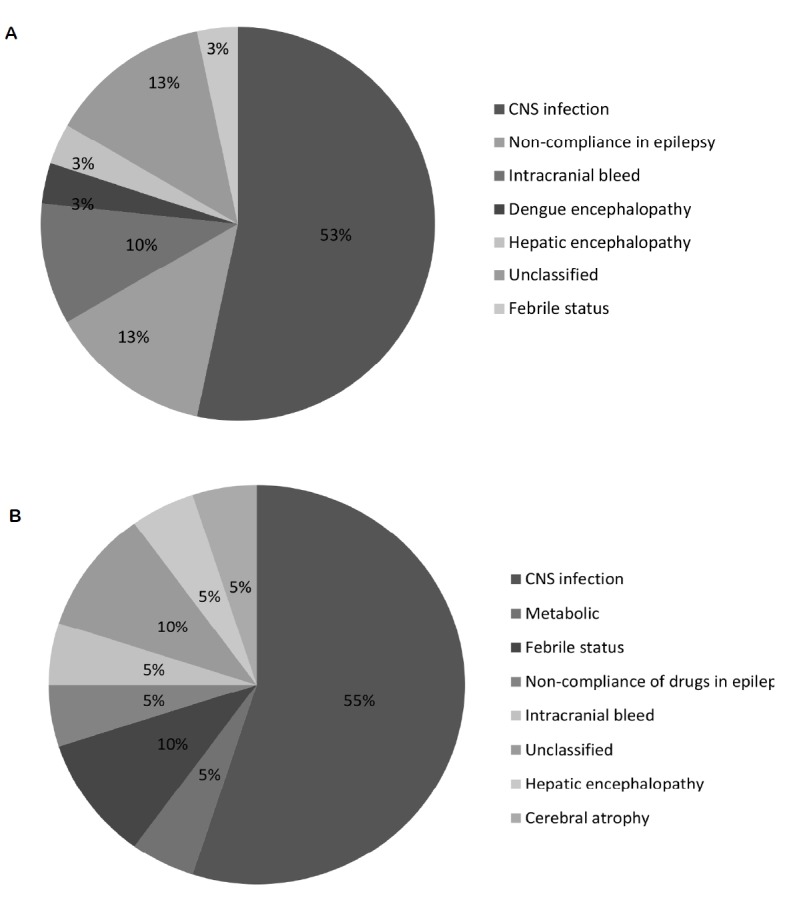
Results: Fifty children (28 males) with CSE were enrolled, of which 20 (40%) progressed to RSE. Central nervous system (CNS) infection was the most common etiology (53% in SE and 55% in RSE, p > 0.05). Non-compliance with anti-epileptic drugs was the second most common etiology. The overall mortality rate was 38%, and although the odds of death in RSE (50%) were higher than in SE (30%), this difference was not statistically significant (p = 0.15). The odds of having a poor outcome was six times higher in children with RSE as compared to those with SE (odds ratio, 6.0; 95% confidence interval, 1.6-22.3; p = 0.005).
Conclusions: When managing CNS infections, pediatricians need to be aware of the high risk of developing RSE. In addition, the possibility of RSE should be considered and managed promptly in an intensive-care setting, to reduce the mortality and morbidity of this severe neurological condition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


