{"title":"代偿性肝硬化:自然病程和疾病改良策略。","authors":"Ramesh Kumar, Sudhir Kumar, Sabbu Surya Prakash","doi":"10.5662/wjm.v13.i4.179","DOIUrl":null,"url":null,"abstract":"<p><p>Compensated liver cirrhosis (CLC) is defined as cirrhosis with one or more decompensating events, such as ascites, variceal haemorrhage, or hepatic encephalopathy. Patients with CLC are largely asymptomatic with preserved hepatic function. The transition from CLC to decompensated cirrhosis occurs as a result of a complex interaction between multiple predisposing and precipitating factors. The first decompensation event in CLC patients is considered a significant turning point in the progression of cirrhosis, as it signals a drastic decline in median survival rates from 10-12 years to only 1-2 years. Furthermore, early cirrhosis has the potential to regress as liver fibrosis is a dynamic condition. With the advent of effective non-invasive tools for detecting hepatic fibrosis, more and more patients with CLC are currently being recognised. This offers clinicians a unique opportunity to properly manage such patients in order to achieve cirrhosis regression or, at the very least, prevent its progression. There are numerous emerging approaches for preventing or delaying decompensation in CLC patients. A growing body of evidence indicates that treating the underlying cause can lead to cirrhosis regression, and the use of non-selective beta-blockers can prevent decompensation by lowering portal hypertension. Additionally, addressing various cofactors (such as obesity, diabetes, dyslipidaemia, and alcoholism) and precipitating factors (such as infection, viral hepatitis, and hepatotoxic drugs) that have a detrimental impact on the natural course of cirrhosis may benefit patients with CLC. However, high-quality data must be generated through well-designed and adequately powered randomised clinical trials to validate these disease-modifying techniques for CLC patients. This article discussed the natural history of CLC, risk factors for its progression, and therapeutic approaches that could alter the trajectory of CLC evolution and improve outcomes.</p>","PeriodicalId":94271,"journal":{"name":"World journal of methodology","volume":"13 4","pages":"179-193"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/eb/49/WJM-13-179.PMC10523240.pdf","citationCount":"0","resultStr":"{\"title\":\"Compensated liver cirrhosis: Natural course and disease-modifying strategies.\",\"authors\":\"Ramesh Kumar, Sudhir Kumar, Sabbu Surya Prakash\",\"doi\":\"10.5662/wjm.v13.i4.179\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Compensated liver cirrhosis (CLC) is defined as cirrhosis with one or more decompensating events, such as ascites, variceal haemorrhage, or hepatic encephalopathy. Patients with CLC are largely asymptomatic with preserved hepatic function. The transition from CLC to decompensated cirrhosis occurs as a result of a complex interaction between multiple predisposing and precipitating factors. The first decompensation event in CLC patients is considered a significant turning point in the progression of cirrhosis, as it signals a drastic decline in median survival rates from 10-12 years to only 1-2 years. Furthermore, early cirrhosis has the potential to regress as liver fibrosis is a dynamic condition. With the advent of effective non-invasive tools for detecting hepatic fibrosis, more and more patients with CLC are currently being recognised. This offers clinicians a unique opportunity to properly manage such patients in order to achieve cirrhosis regression or, at the very least, prevent its progression. There are numerous emerging approaches for preventing or delaying decompensation in CLC patients. A growing body of evidence indicates that treating the underlying cause can lead to cirrhosis regression, and the use of non-selective beta-blockers can prevent decompensation by lowering portal hypertension. Additionally, addressing various cofactors (such as obesity, diabetes, dyslipidaemia, and alcoholism) and precipitating factors (such as infection, viral hepatitis, and hepatotoxic drugs) that have a detrimental impact on the natural course of cirrhosis may benefit patients with CLC. However, high-quality data must be generated through well-designed and adequately powered randomised clinical trials to validate these disease-modifying techniques for CLC patients. This article discussed the natural history of CLC, risk factors for its progression, and therapeutic approaches that could alter the trajectory of CLC evolution and improve outcomes.</p>\",\"PeriodicalId\":94271,\"journal\":{\"name\":\"World journal of methodology\",\"volume\":\"13 4\",\"pages\":\"179-193\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/eb/49/WJM-13-179.PMC10523240.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of methodology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5662/wjm.v13.i4.179\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of methodology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5662/wjm.v13.i4.179","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Compensated liver cirrhosis: Natural course and disease-modifying strategies.
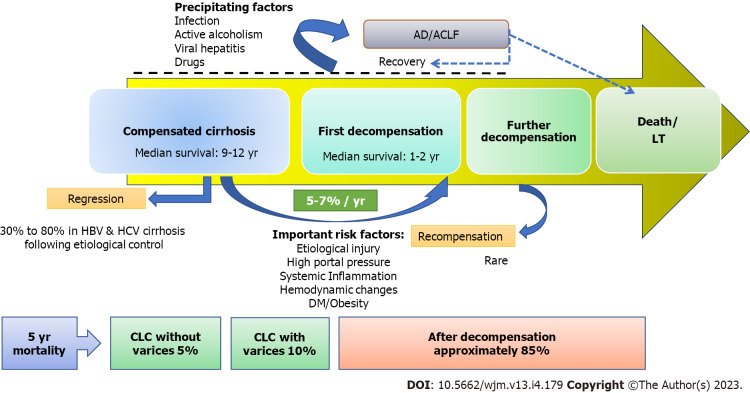
Compensated liver cirrhosis (CLC) is defined as cirrhosis with one or more decompensating events, such as ascites, variceal haemorrhage, or hepatic encephalopathy. Patients with CLC are largely asymptomatic with preserved hepatic function. The transition from CLC to decompensated cirrhosis occurs as a result of a complex interaction between multiple predisposing and precipitating factors. The first decompensation event in CLC patients is considered a significant turning point in the progression of cirrhosis, as it signals a drastic decline in median survival rates from 10-12 years to only 1-2 years. Furthermore, early cirrhosis has the potential to regress as liver fibrosis is a dynamic condition. With the advent of effective non-invasive tools for detecting hepatic fibrosis, more and more patients with CLC are currently being recognised. This offers clinicians a unique opportunity to properly manage such patients in order to achieve cirrhosis regression or, at the very least, prevent its progression. There are numerous emerging approaches for preventing or delaying decompensation in CLC patients. A growing body of evidence indicates that treating the underlying cause can lead to cirrhosis regression, and the use of non-selective beta-blockers can prevent decompensation by lowering portal hypertension. Additionally, addressing various cofactors (such as obesity, diabetes, dyslipidaemia, and alcoholism) and precipitating factors (such as infection, viral hepatitis, and hepatotoxic drugs) that have a detrimental impact on the natural course of cirrhosis may benefit patients with CLC. However, high-quality data must be generated through well-designed and adequately powered randomised clinical trials to validate these disease-modifying techniques for CLC patients. This article discussed the natural history of CLC, risk factors for its progression, and therapeutic approaches that could alter the trajectory of CLC evolution and improve outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


