Kieran Jd Steer, Zhuolu Sun, Daniel C Sadowski, Jean H E Yong, Andrew Coldman, Nicole Nemecek, Huiming Yang
{"title":"低风险腺瘤切除后停止结肠镜检查对临床结果和医疗资源的影响:一项使用OncoSim结肠直肠模型的模拟研究。","authors":"Kieran Jd Steer, Zhuolu Sun, Daniel C Sadowski, Jean H E Yong, Andrew Coldman, Nicole Nemecek, Huiming Yang","doi":"10.1177/09691413231202877","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To estimate the impact on clinical outcomes and healthcare resource use from recommending that patients with 1-2 low-risk adenomas (LRAs) return to routine fecal immunochemical test (FIT) screening instead of surveillance colonoscopy, from a Canadian provincial healthcare system perspective.</p><p><strong>Methods: </strong>The OncoSim-Colorectal microsimulation model simulated average-risk individuals eligible for FIT-based colorectal cancer (CRC) screening in Alberta, Canada. We simulated two surveillance strategies that applied to individuals with 1-2 LRAs (<10 mm) removed as part of the average risk CRC screening program: (a) Surveillance colonoscopy (status quo) and (b) return to FIT screening (new strategy); both at 5 years after polypectomy. A 75 ng/mL FIT positivity threshold was used in the base case. The simulations projected average annual CRC outcomes and healthcare resource use from 2023 to 2042. We conducted alternative scenarios and sensitivity analyses on key variables.</p><p><strong>Results: </strong>Returning to FIT screening (versus surveillance colonoscopy) after polypectomy was projected to have minimal impact on long-term CRC incidence and deaths (not statistically significant). There was a projected decrease of one (4%) major bleeding event and seven (5%) perforation events per year. There was a projected increase of 4800 (1.5%) FIT screens, decrease of 3900 (5.1%) colonoscopies, and a decrease of $3.4 million (1.2%) in total healthcare costs per year, on average. The annual colonoscopies averted and healthcare cost savings increased over time. Results were similar in the alternative scenarios and sensitivity analyses.</p><p><strong>Conclusions: </strong>Returning to FIT screening would have similar clinical outcomes as surveillance colonoscopy but could reduce colonoscopy demand and healthcare costs.</p>","PeriodicalId":51089,"journal":{"name":"Journal of Medical Screening","volume":" ","pages":"78-84"},"PeriodicalIF":2.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11083724/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact on clinical outcomes and healthcare resources from discontinuing colonoscopy surveillance subsequent to low-risk adenoma removal: A simulation study using the OncoSim-Colorectal model.\",\"authors\":\"Kieran Jd Steer, Zhuolu Sun, Daniel C Sadowski, Jean H E Yong, Andrew Coldman, Nicole Nemecek, Huiming Yang\",\"doi\":\"10.1177/09691413231202877\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To estimate the impact on clinical outcomes and healthcare resource use from recommending that patients with 1-2 low-risk adenomas (LRAs) return to routine fecal immunochemical test (FIT) screening instead of surveillance colonoscopy, from a Canadian provincial healthcare system perspective.</p><p><strong>Methods: </strong>The OncoSim-Colorectal microsimulation model simulated average-risk individuals eligible for FIT-based colorectal cancer (CRC) screening in Alberta, Canada. We simulated two surveillance strategies that applied to individuals with 1-2 LRAs (<10 mm) removed as part of the average risk CRC screening program: (a) Surveillance colonoscopy (status quo) and (b) return to FIT screening (new strategy); both at 5 years after polypectomy. A 75 ng/mL FIT positivity threshold was used in the base case. The simulations projected average annual CRC outcomes and healthcare resource use from 2023 to 2042. We conducted alternative scenarios and sensitivity analyses on key variables.</p><p><strong>Results: </strong>Returning to FIT screening (versus surveillance colonoscopy) after polypectomy was projected to have minimal impact on long-term CRC incidence and deaths (not statistically significant). There was a projected decrease of one (4%) major bleeding event and seven (5%) perforation events per year. There was a projected increase of 4800 (1.5%) FIT screens, decrease of 3900 (5.1%) colonoscopies, and a decrease of $3.4 million (1.2%) in total healthcare costs per year, on average. The annual colonoscopies averted and healthcare cost savings increased over time. Results were similar in the alternative scenarios and sensitivity analyses.</p><p><strong>Conclusions: </strong>Returning to FIT screening would have similar clinical outcomes as surveillance colonoscopy but could reduce colonoscopy demand and healthcare costs.</p>\",\"PeriodicalId\":51089,\"journal\":{\"name\":\"Journal of Medical Screening\",\"volume\":\" \",\"pages\":\"78-84\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11083724/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Screening\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/09691413231202877\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Screening","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/09691413231202877","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
The impact on clinical outcomes and healthcare resources from discontinuing colonoscopy surveillance subsequent to low-risk adenoma removal: A simulation study using the OncoSim-Colorectal model.
Objective: To estimate the impact on clinical outcomes and healthcare resource use from recommending that patients with 1-2 low-risk adenomas (LRAs) return to routine fecal immunochemical test (FIT) screening instead of surveillance colonoscopy, from a Canadian provincial healthcare system perspective.
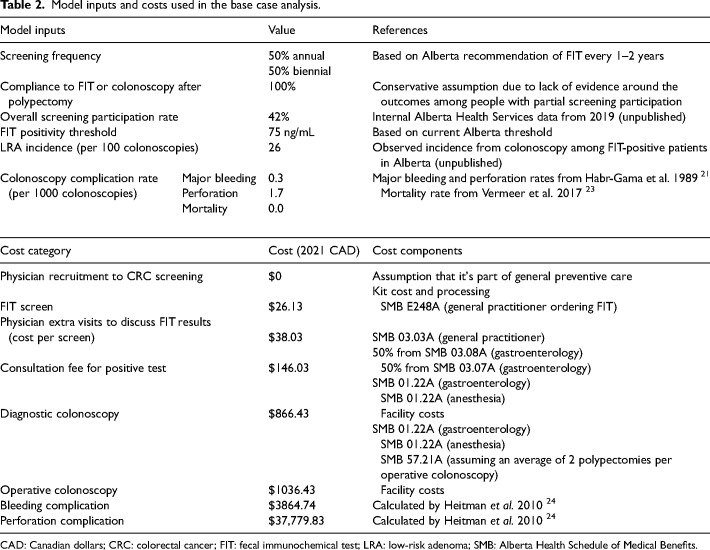
Methods: The OncoSim-Colorectal microsimulation model simulated average-risk individuals eligible for FIT-based colorectal cancer (CRC) screening in Alberta, Canada. We simulated two surveillance strategies that applied to individuals with 1-2 LRAs (<10 mm) removed as part of the average risk CRC screening program: (a) Surveillance colonoscopy (status quo) and (b) return to FIT screening (new strategy); both at 5 years after polypectomy. A 75 ng/mL FIT positivity threshold was used in the base case. The simulations projected average annual CRC outcomes and healthcare resource use from 2023 to 2042. We conducted alternative scenarios and sensitivity analyses on key variables.
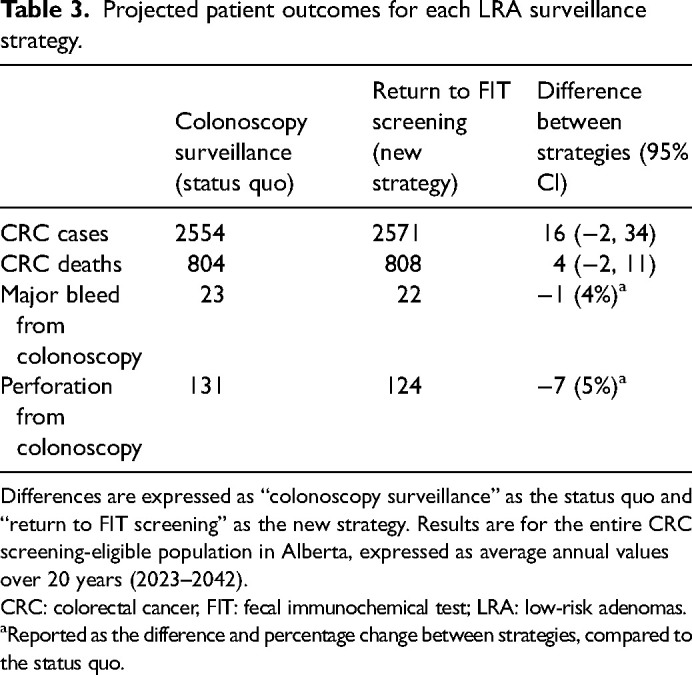
Results: Returning to FIT screening (versus surveillance colonoscopy) after polypectomy was projected to have minimal impact on long-term CRC incidence and deaths (not statistically significant). There was a projected decrease of one (4%) major bleeding event and seven (5%) perforation events per year. There was a projected increase of 4800 (1.5%) FIT screens, decrease of 3900 (5.1%) colonoscopies, and a decrease of $3.4 million (1.2%) in total healthcare costs per year, on average. The annual colonoscopies averted and healthcare cost savings increased over time. Results were similar in the alternative scenarios and sensitivity analyses.
Conclusions: Returning to FIT screening would have similar clinical outcomes as surveillance colonoscopy but could reduce colonoscopy demand and healthcare costs.
期刊介绍:
Journal of Medical Screening, a fully peer reviewed journal, is concerned with all aspects of medical screening, particularly the publication of research that advances screening theory and practice. The journal aims to increase awareness of the principles of screening (quantitative and statistical aspects), screening techniques and procedures and methodologies from all specialties. An essential subscription for physicians, clinicians and academics with an interest in screening, epidemiology and public health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


