Tara C Cosgrove, Robert J Gajarski, Kevin F Dolan, Stephen A Hart, Kaitlin E L'Italien, Stacy Kuehn, Stephanie Ishmael, Jessica L Bowman, Jill A Fitch, Brittney K Hills, Ryan S Bode
{"title":"提高情境意识以减少住院儿科心脏病患者的紧急ICU转移。","authors":"Tara C Cosgrove, Robert J Gajarski, Kevin F Dolan, Stephen A Hart, Kaitlin E L'Italien, Stacy Kuehn, Stephanie Ishmael, Jessica L Bowman, Jill A Fitch, Brittney K Hills, Ryan S Bode","doi":"10.1097/pq9.0000000000000630","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Failure to recognize and mitigate critical patient deterioration remains a source of serious preventable harm to hospitalized pediatric cardiac patients. Emergency transfers (ETs) occur 10-20 times more often than code events outside the intensive care unit (ICU) and are associated with morbidity and mortality. This quality improvement project aimed to increase days between ETs and code events on an acute care cardiology unit (ACCU) from a baseline median of 17 and 32 days to ≥70 and 90 days within 12 months.</p><p><strong>Methods: </strong>Institutional leaders, cardiology-trained physicians and nurses, and trainees convened, utilizing the Institution for Healthcare Improvement model to achieve the project aims. Interventions implemented focused on improving situational awareness (SA), including a \"Must Call List,\" evening rounds, a visual management board, and daily huddles. Outcome measures included calendar days between ETs and code events in the ACCU. Process measures tracked the utilization of interventions, and cardiac ICU length of stay was a balancing measure. Statistical process control chart methodology was utilized to analyze the impact of interventions.</p><p><strong>Results: </strong>Within the study period, we observed a centerline shift in primary outcome measures with an increase from 17 to 56 days between ETs and 32 to 62 days between code events in the ACCU, with sustained improvement. Intervention utilization ranged from 87% to 100%, and there was no observed special cause variation in our balancing measure.</p><p><strong>Conclusions: </strong>Interventions focused on improving SA in a particularly vulnerable patient population led to sustained improvement with reduced ETs and code events outside the ICU.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 5","pages":"e630"},"PeriodicalIF":1.2000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/fd/pqs-8-e630.PMC10538891.pdf","citationCount":"0","resultStr":"{\"title\":\"Improving Situational Awareness to Decrease Emergency ICU Transfers for Hospitalized Pediatric Cardiology Patients.\",\"authors\":\"Tara C Cosgrove, Robert J Gajarski, Kevin F Dolan, Stephen A Hart, Kaitlin E L'Italien, Stacy Kuehn, Stephanie Ishmael, Jessica L Bowman, Jill A Fitch, Brittney K Hills, Ryan S Bode\",\"doi\":\"10.1097/pq9.0000000000000630\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Failure to recognize and mitigate critical patient deterioration remains a source of serious preventable harm to hospitalized pediatric cardiac patients. Emergency transfers (ETs) occur 10-20 times more often than code events outside the intensive care unit (ICU) and are associated with morbidity and mortality. This quality improvement project aimed to increase days between ETs and code events on an acute care cardiology unit (ACCU) from a baseline median of 17 and 32 days to ≥70 and 90 days within 12 months.</p><p><strong>Methods: </strong>Institutional leaders, cardiology-trained physicians and nurses, and trainees convened, utilizing the Institution for Healthcare Improvement model to achieve the project aims. Interventions implemented focused on improving situational awareness (SA), including a \\\"Must Call List,\\\" evening rounds, a visual management board, and daily huddles. Outcome measures included calendar days between ETs and code events in the ACCU. Process measures tracked the utilization of interventions, and cardiac ICU length of stay was a balancing measure. Statistical process control chart methodology was utilized to analyze the impact of interventions.</p><p><strong>Results: </strong>Within the study period, we observed a centerline shift in primary outcome measures with an increase from 17 to 56 days between ETs and 32 to 62 days between code events in the ACCU, with sustained improvement. Intervention utilization ranged from 87% to 100%, and there was no observed special cause variation in our balancing measure.</p><p><strong>Conclusions: </strong>Interventions focused on improving SA in a particularly vulnerable patient population led to sustained improvement with reduced ETs and code events outside the ICU.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"8 5\",\"pages\":\"e630\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/fd/pqs-8-e630.PMC10538891.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000630\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000630","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Improving Situational Awareness to Decrease Emergency ICU Transfers for Hospitalized Pediatric Cardiology Patients.
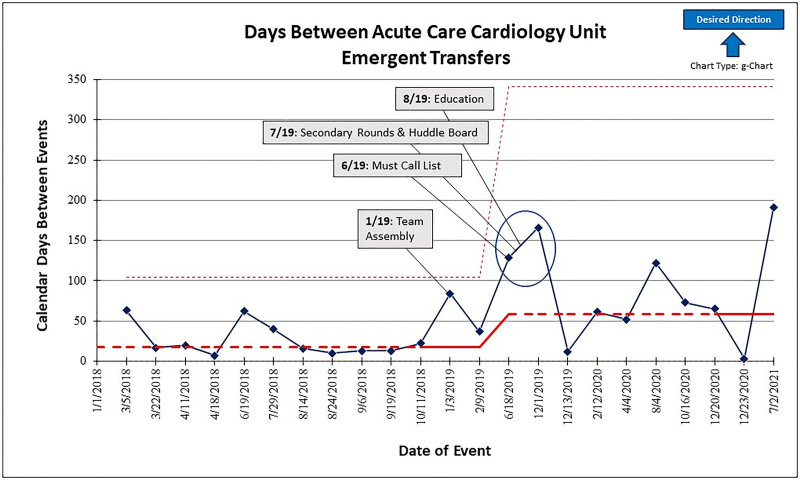
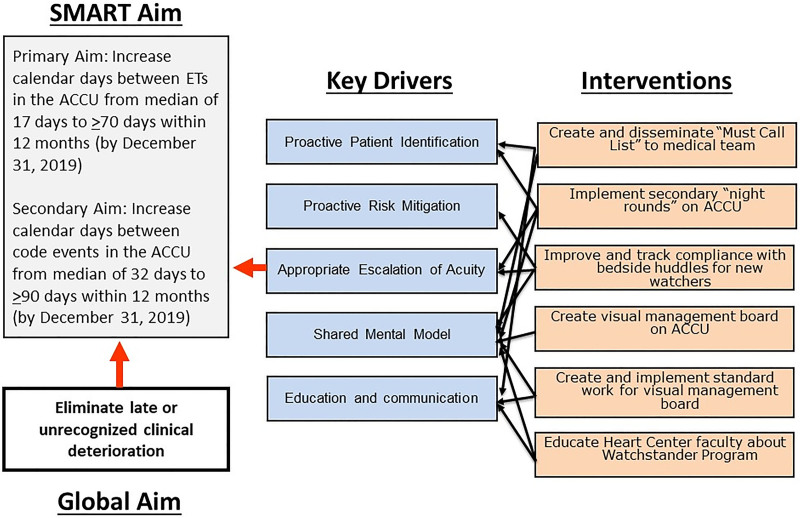
Introduction: Failure to recognize and mitigate critical patient deterioration remains a source of serious preventable harm to hospitalized pediatric cardiac patients. Emergency transfers (ETs) occur 10-20 times more often than code events outside the intensive care unit (ICU) and are associated with morbidity and mortality. This quality improvement project aimed to increase days between ETs and code events on an acute care cardiology unit (ACCU) from a baseline median of 17 and 32 days to ≥70 and 90 days within 12 months.
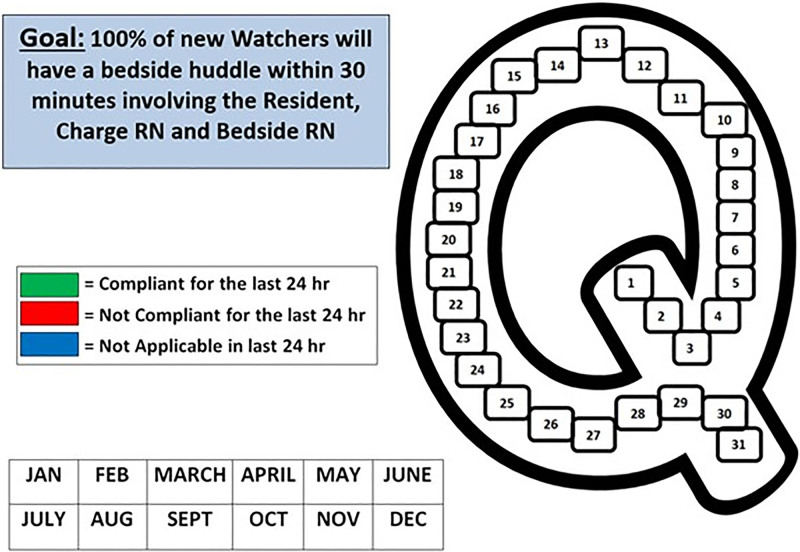
Methods: Institutional leaders, cardiology-trained physicians and nurses, and trainees convened, utilizing the Institution for Healthcare Improvement model to achieve the project aims. Interventions implemented focused on improving situational awareness (SA), including a "Must Call List," evening rounds, a visual management board, and daily huddles. Outcome measures included calendar days between ETs and code events in the ACCU. Process measures tracked the utilization of interventions, and cardiac ICU length of stay was a balancing measure. Statistical process control chart methodology was utilized to analyze the impact of interventions.
Results: Within the study period, we observed a centerline shift in primary outcome measures with an increase from 17 to 56 days between ETs and 32 to 62 days between code events in the ACCU, with sustained improvement. Intervention utilization ranged from 87% to 100%, and there was no observed special cause variation in our balancing measure.
Conclusions: Interventions focused on improving SA in a particularly vulnerable patient population led to sustained improvement with reduced ETs and code events outside the ICU.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


