Smitha Israel, Sofia Perazzo, Morgan Lee, Rachel Samson, Parissa Safari-Ferra, Ranjodh Badh, Solomon Abera, Lamia Soghier
{"title":"改进NICU疼痛管理干预后疼痛再评估的记录。","authors":"Smitha Israel, Sofia Perazzo, Morgan Lee, Rachel Samson, Parissa Safari-Ferra, Ranjodh Badh, Solomon Abera, Lamia Soghier","doi":"10.1097/pq9.0000000000000688","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neonates exposed to painful procedures require pain assessment and reassessment using nonverbal scales. Nurses perform initial assessments routinely, but reassessment is variable. The goal was to increase pain reassessments in neonates with a previous score of 4 or higher within 60 minutes from 50% to 75% within 12 months.</p><p><strong>Methods: </strong>After identifying key drivers, we tested several interventions using the IHI's Model for Improvement. The outcome measure was the rate of reassessments within 1 hour after scoring ≥4 on the Neonatal Pain Agitation and Sedation Scale (N-PASS). Duration of time between scoring and intervention was documented. Interventions included electronic health record (EHR) changes, direct communication with bedside nurses through text messages and emails, in-person education, and a yearly competency module. The process measure was the number of messages/emails to staff. Sedation scores were the balancing measure.</p><p><strong>Results: </strong>Baseline compliance was 50% with significant variability. A centerline shift occurred after the first intervention. After the first four interventions in the following 3 months, a 29% total increase occurred. Overall time-lapse between reassessments decreased from 102 to 90 minutes. Overall sedation scores decreased from -2.5 during the baseline to -1.7 during the sustain period. The goal of 75% pain reassessments was achieved and sustained for two years.</p><p><strong>Conclusions: </strong>Automated tools such as the trigger report provided data that increased noncompliance visibility. Real-time and personalized reminders and education improved awareness and set the tone for culture change. Electronic health record reminders for reassessments and standardized annual education helped in sustaining change.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 5","pages":"e688"},"PeriodicalIF":1.2000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10538901/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improving Documentation of Pain Reassessment after Pain Management Interventions in the NICU.\",\"authors\":\"Smitha Israel, Sofia Perazzo, Morgan Lee, Rachel Samson, Parissa Safari-Ferra, Ranjodh Badh, Solomon Abera, Lamia Soghier\",\"doi\":\"10.1097/pq9.0000000000000688\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neonates exposed to painful procedures require pain assessment and reassessment using nonverbal scales. Nurses perform initial assessments routinely, but reassessment is variable. The goal was to increase pain reassessments in neonates with a previous score of 4 or higher within 60 minutes from 50% to 75% within 12 months.</p><p><strong>Methods: </strong>After identifying key drivers, we tested several interventions using the IHI's Model for Improvement. The outcome measure was the rate of reassessments within 1 hour after scoring ≥4 on the Neonatal Pain Agitation and Sedation Scale (N-PASS). Duration of time between scoring and intervention was documented. Interventions included electronic health record (EHR) changes, direct communication with bedside nurses through text messages and emails, in-person education, and a yearly competency module. The process measure was the number of messages/emails to staff. Sedation scores were the balancing measure.</p><p><strong>Results: </strong>Baseline compliance was 50% with significant variability. A centerline shift occurred after the first intervention. After the first four interventions in the following 3 months, a 29% total increase occurred. Overall time-lapse between reassessments decreased from 102 to 90 minutes. Overall sedation scores decreased from -2.5 during the baseline to -1.7 during the sustain period. The goal of 75% pain reassessments was achieved and sustained for two years.</p><p><strong>Conclusions: </strong>Automated tools such as the trigger report provided data that increased noncompliance visibility. Real-time and personalized reminders and education improved awareness and set the tone for culture change. Electronic health record reminders for reassessments and standardized annual education helped in sustaining change.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"8 5\",\"pages\":\"e688\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10538901/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000688\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000688","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Improving Documentation of Pain Reassessment after Pain Management Interventions in the NICU.
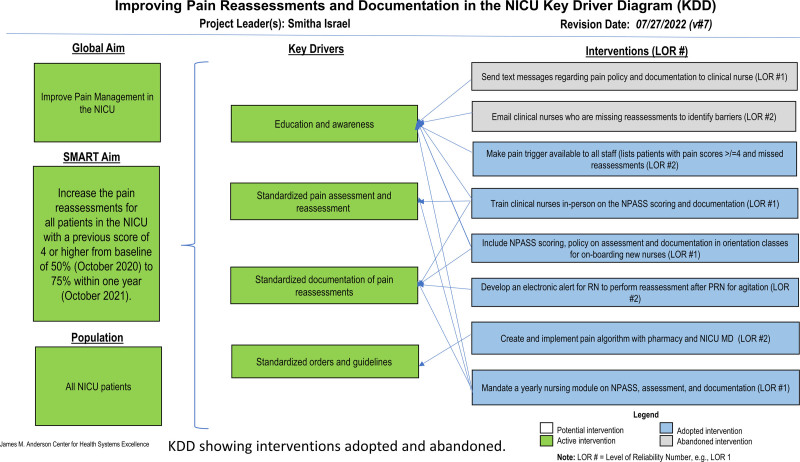
Background: Neonates exposed to painful procedures require pain assessment and reassessment using nonverbal scales. Nurses perform initial assessments routinely, but reassessment is variable. The goal was to increase pain reassessments in neonates with a previous score of 4 or higher within 60 minutes from 50% to 75% within 12 months.
Methods: After identifying key drivers, we tested several interventions using the IHI's Model for Improvement. The outcome measure was the rate of reassessments within 1 hour after scoring ≥4 on the Neonatal Pain Agitation and Sedation Scale (N-PASS). Duration of time between scoring and intervention was documented. Interventions included electronic health record (EHR) changes, direct communication with bedside nurses through text messages and emails, in-person education, and a yearly competency module. The process measure was the number of messages/emails to staff. Sedation scores were the balancing measure.
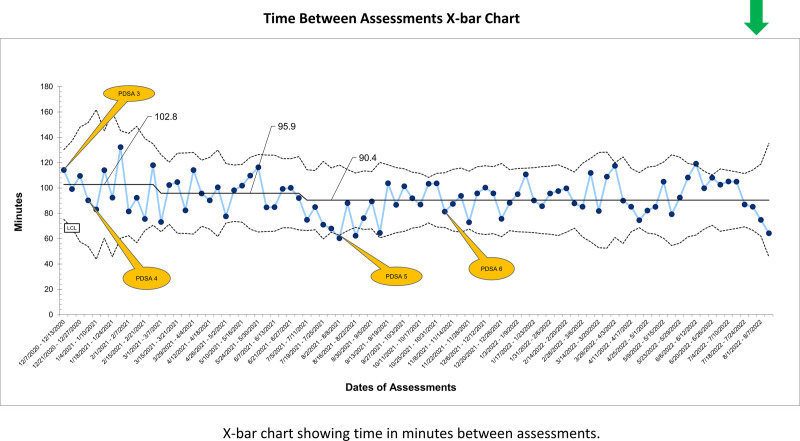
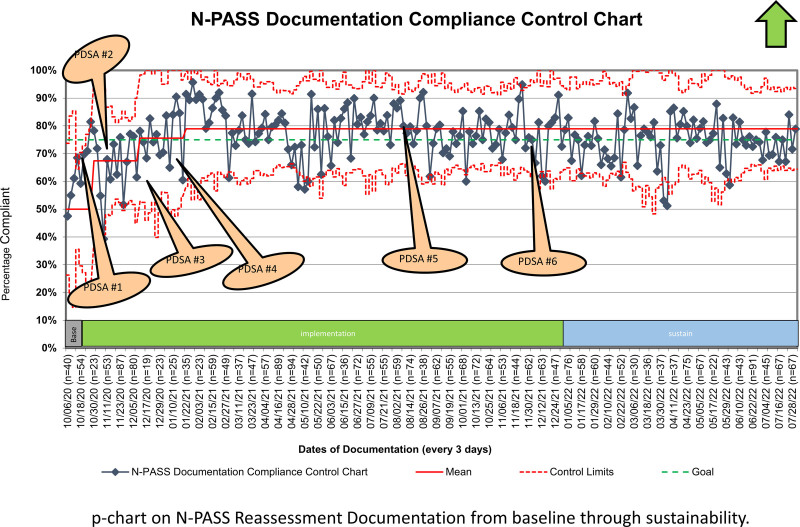
Results: Baseline compliance was 50% with significant variability. A centerline shift occurred after the first intervention. After the first four interventions in the following 3 months, a 29% total increase occurred. Overall time-lapse between reassessments decreased from 102 to 90 minutes. Overall sedation scores decreased from -2.5 during the baseline to -1.7 during the sustain period. The goal of 75% pain reassessments was achieved and sustained for two years.
Conclusions: Automated tools such as the trigger report provided data that increased noncompliance visibility. Real-time and personalized reminders and education improved awareness and set the tone for culture change. Electronic health record reminders for reassessments and standardized annual education helped in sustaining change.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


