Shabin Fahad, Sayali Shirsath, Matthew Metcalfe, Ahmed Elmallah
{"title":"高龄患者颈动脉内膜切除术:短期、中期和长期疗效。","authors":"Shabin Fahad, Sayali Shirsath, Matthew Metcalfe, Ahmed Elmallah","doi":"10.5758/vsi.230060","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>: Carotid endarterectomy (CEA) has an established effect on stroke-free survival in patients with carotid artery stenosis. Most landmark trials excluded patients ≥80 years of age due to their perceived high risk and uncertainty regarding the benefits of CEA. Despite the ongoing global increase in life expectancy, guidelines have not changed. The current study aimed to assess CEA outcomes in patients ≥80 years of age.</p><p><strong>Materials and methods: </strong>: Data from patients ≥80 years of age, who underwent CEA between April 2016 and April 2022, were collected. Demographic information, comorbidities, surgical details, operative details, outcomes, and post-CEA survival were reviewed, and long-term data up to April 2023 were collected.</p><p><strong>Results: </strong>: Over the 6-year study period, 258 CEA procedures were recorded, of which 70 (27.1%) were performed in patients ≥80 years of age; the mean age was 84 years (range, 80-96 years), 47 (67.1%) were males, and 69 (98.6%) were symptomatic. Twenty-three (32.9%) patients were American Society of Anesthesiologists (ASA) grade 2, and 47 (67.1%) were grade 3. The 30-day stroke and mortality rates were 4.3% and 1.4%, respectively. At 1, 3, and 5 years, the cumulative freedom-from-stroke rates were 95.7%, 92.9%, and 91.4%, respectively, and the cumulative survival rates were 94.3%, 75.7%, and 61.4%, respectively. No risk factors affected early or late stroke or early mortality rates. Patients with ASA grade 3 had significantly lower cumulative survival than those with grade 2 (HR, 5.29; 95% CI, 1.590-17.603; P<0.01).</p><p><strong>Conclusion: </strong>: CEA was safe and effective in average-risk, elderly patients. Higher risk patients (i.e., ASA 3) showed no increased 30-day risk for stroke or mortality but exhibited significantly worse long-term survival. Hence, careful consideration of the benefits before performing CEA is crucial.</p>","PeriodicalId":52311,"journal":{"name":"Vascular Specialist International","volume":"39 ","pages":"28"},"PeriodicalIF":0.8000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/5f/vsi-39-28.PMC10519940.pdf","citationCount":"0","resultStr":"{\"title\":\"Carotid Endarterectomy in the Very Elderly: Short-, Medium-, and Long-Term Outcomes.\",\"authors\":\"Shabin Fahad, Sayali Shirsath, Matthew Metcalfe, Ahmed Elmallah\",\"doi\":\"10.5758/vsi.230060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>: Carotid endarterectomy (CEA) has an established effect on stroke-free survival in patients with carotid artery stenosis. Most landmark trials excluded patients ≥80 years of age due to their perceived high risk and uncertainty regarding the benefits of CEA. Despite the ongoing global increase in life expectancy, guidelines have not changed. The current study aimed to assess CEA outcomes in patients ≥80 years of age.</p><p><strong>Materials and methods: </strong>: Data from patients ≥80 years of age, who underwent CEA between April 2016 and April 2022, were collected. Demographic information, comorbidities, surgical details, operative details, outcomes, and post-CEA survival were reviewed, and long-term data up to April 2023 were collected.</p><p><strong>Results: </strong>: Over the 6-year study period, 258 CEA procedures were recorded, of which 70 (27.1%) were performed in patients ≥80 years of age; the mean age was 84 years (range, 80-96 years), 47 (67.1%) were males, and 69 (98.6%) were symptomatic. Twenty-three (32.9%) patients were American Society of Anesthesiologists (ASA) grade 2, and 47 (67.1%) were grade 3. The 30-day stroke and mortality rates were 4.3% and 1.4%, respectively. At 1, 3, and 5 years, the cumulative freedom-from-stroke rates were 95.7%, 92.9%, and 91.4%, respectively, and the cumulative survival rates were 94.3%, 75.7%, and 61.4%, respectively. No risk factors affected early or late stroke or early mortality rates. Patients with ASA grade 3 had significantly lower cumulative survival than those with grade 2 (HR, 5.29; 95% CI, 1.590-17.603; P<0.01).</p><p><strong>Conclusion: </strong>: CEA was safe and effective in average-risk, elderly patients. Higher risk patients (i.e., ASA 3) showed no increased 30-day risk for stroke or mortality but exhibited significantly worse long-term survival. Hence, careful consideration of the benefits before performing CEA is crucial.</p>\",\"PeriodicalId\":52311,\"journal\":{\"name\":\"Vascular Specialist International\",\"volume\":\"39 \",\"pages\":\"28\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/5f/vsi-39-28.PMC10519940.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vascular Specialist International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5758/vsi.230060\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular Specialist International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5758/vsi.230060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Carotid Endarterectomy in the Very Elderly: Short-, Medium-, and Long-Term Outcomes.
Purpose: : Carotid endarterectomy (CEA) has an established effect on stroke-free survival in patients with carotid artery stenosis. Most landmark trials excluded patients ≥80 years of age due to their perceived high risk and uncertainty regarding the benefits of CEA. Despite the ongoing global increase in life expectancy, guidelines have not changed. The current study aimed to assess CEA outcomes in patients ≥80 years of age.
Materials and methods: : Data from patients ≥80 years of age, who underwent CEA between April 2016 and April 2022, were collected. Demographic information, comorbidities, surgical details, operative details, outcomes, and post-CEA survival were reviewed, and long-term data up to April 2023 were collected.
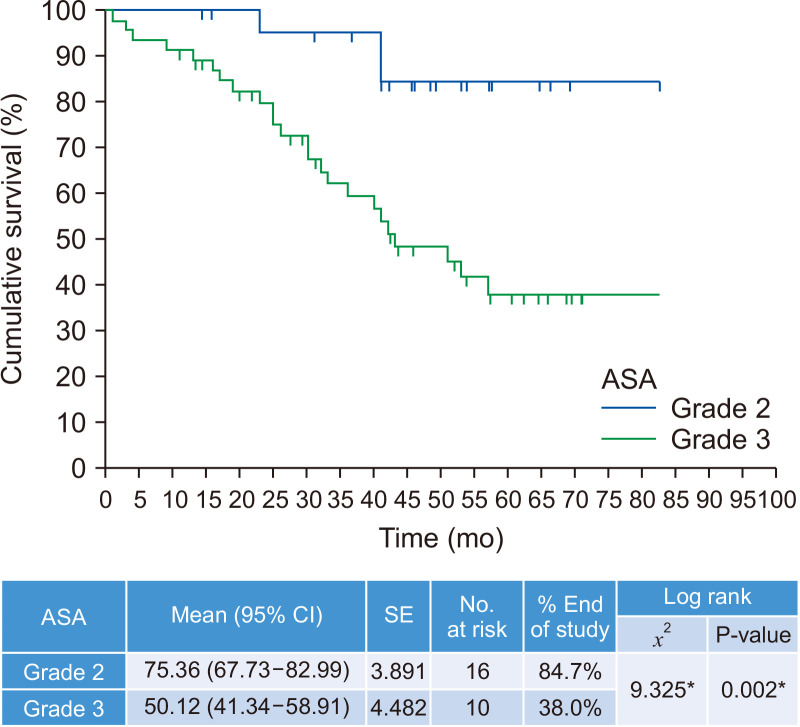
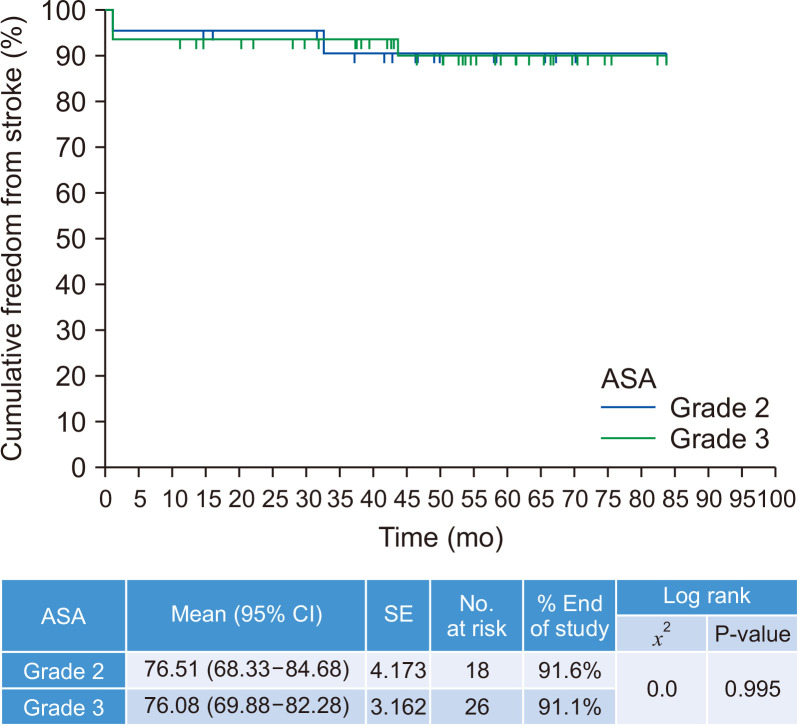
Results: : Over the 6-year study period, 258 CEA procedures were recorded, of which 70 (27.1%) were performed in patients ≥80 years of age; the mean age was 84 years (range, 80-96 years), 47 (67.1%) were males, and 69 (98.6%) were symptomatic. Twenty-three (32.9%) patients were American Society of Anesthesiologists (ASA) grade 2, and 47 (67.1%) were grade 3. The 30-day stroke and mortality rates were 4.3% and 1.4%, respectively. At 1, 3, and 5 years, the cumulative freedom-from-stroke rates were 95.7%, 92.9%, and 91.4%, respectively, and the cumulative survival rates were 94.3%, 75.7%, and 61.4%, respectively. No risk factors affected early or late stroke or early mortality rates. Patients with ASA grade 3 had significantly lower cumulative survival than those with grade 2 (HR, 5.29; 95% CI, 1.590-17.603; P<0.01).
Conclusion: : CEA was safe and effective in average-risk, elderly patients. Higher risk patients (i.e., ASA 3) showed no increased 30-day risk for stroke or mortality but exhibited significantly worse long-term survival. Hence, careful consideration of the benefits before performing CEA is crucial.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


