Ashish K Khanna, Marilyn A Moucharite, Patrick J Benefield, Roop Kaw
{"title":"与非计划医疗和外科重症监护室入院相关的患者特征、临床和经济结果:回顾性分析。","authors":"Ashish K Khanna, Marilyn A Moucharite, Patrick J Benefield, Roop Kaw","doi":"10.2147/CEOR.S424759","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To characterize medical and surgical patient characteristics, as well as clinical and economic outcomes, associated with unplanned intensive care unit (ICU) admissions.</p><p><strong>Patients and methods: </strong>This was a retrospective matched cohort analysis that utilized the PINC AI<sup>TM</sup> Healthcare Database, which collects deidentified data from 25% of United States (US) hospital admissions. Discharge records were assessed for medical and surgical admissions in 2021. An unplanned ICU admission was defined as direct transfer from a medical, surgical, or telemetry unit to the ICU. Patients with and without an unplanned ICU admission were 1:1 propensity score matched. Differences between patients with and without unplanned ICU admissions were assessed using two-sample <i>t</i>-tests for continuous measures and Chi-square tests for categorical measures.</p><p><strong>Results: </strong>A total of 3,807,124 qualifying admissions were identified. Medical admissions with unplanned ICU transfers were more likely to be urgent/emergent (odds ratio [OR] 2.9, 95% confidence interval [CI 2.7-3.0], p<0.0001), with patient characteristics including male sex (1.4, [1.4-1.4], p<0.0001), obesity (1.7, [1.6-1.7], p<0.0001), and increased Charlson Comorbidity Index (CCI=1: 1.8, [1.8-1.9], p<0.0001; CCI≥5: 3.2, [3.1-3.3], p<0.0001). Surgical admissions with unplanned ICU transfers were more likely to be urgent/emergent (3.1, [2.9-3.2], p<0.0001) and with patients of higher CCI (2.5, [2.3-2.6], p<0.0001 to a CCI of≥5 (7.9, [7.4-8.4], p<0.0001). Between matched medical patients, mean differences in length of stay, cost, and mortality were 4.1 days (p<0.0001), $13,424 (p<0.0001), and 21% (p<0.0001), respectively. Between matched surgical patients, mean differences in these outcomes were 6.4 days (p<0.0001), $21,448 (p<0.0001), and 14% (p<0.0001), respectively.</p><p><strong>Conclusion: </strong>Emergency care in patients with a higher co-morbid burden is more likely to lead to unplanned ICU admission, putting patients at a significantly increased chance of mortality, longer length of stay, and increased costs. Improving care and monitoring of patients outside the ICU may help detect early changes in pathophysiology and enable early intervention.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"703-719"},"PeriodicalIF":2.1000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/ac/ceor-15-703.PMC10541084.pdf","citationCount":"0","resultStr":"{\"title\":\"Patient Characteristics and Clinical and Economic Outcomes Associated with Unplanned Medical and Surgical Intensive Care Unit Admissions: A Retrospective Analysis.\",\"authors\":\"Ashish K Khanna, Marilyn A Moucharite, Patrick J Benefield, Roop Kaw\",\"doi\":\"10.2147/CEOR.S424759\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To characterize medical and surgical patient characteristics, as well as clinical and economic outcomes, associated with unplanned intensive care unit (ICU) admissions.</p><p><strong>Patients and methods: </strong>This was a retrospective matched cohort analysis that utilized the PINC AI<sup>TM</sup> Healthcare Database, which collects deidentified data from 25% of United States (US) hospital admissions. Discharge records were assessed for medical and surgical admissions in 2021. An unplanned ICU admission was defined as direct transfer from a medical, surgical, or telemetry unit to the ICU. Patients with and without an unplanned ICU admission were 1:1 propensity score matched. Differences between patients with and without unplanned ICU admissions were assessed using two-sample <i>t</i>-tests for continuous measures and Chi-square tests for categorical measures.</p><p><strong>Results: </strong>A total of 3,807,124 qualifying admissions were identified. Medical admissions with unplanned ICU transfers were more likely to be urgent/emergent (odds ratio [OR] 2.9, 95% confidence interval [CI 2.7-3.0], p<0.0001), with patient characteristics including male sex (1.4, [1.4-1.4], p<0.0001), obesity (1.7, [1.6-1.7], p<0.0001), and increased Charlson Comorbidity Index (CCI=1: 1.8, [1.8-1.9], p<0.0001; CCI≥5: 3.2, [3.1-3.3], p<0.0001). Surgical admissions with unplanned ICU transfers were more likely to be urgent/emergent (3.1, [2.9-3.2], p<0.0001) and with patients of higher CCI (2.5, [2.3-2.6], p<0.0001 to a CCI of≥5 (7.9, [7.4-8.4], p<0.0001). Between matched medical patients, mean differences in length of stay, cost, and mortality were 4.1 days (p<0.0001), $13,424 (p<0.0001), and 21% (p<0.0001), respectively. Between matched surgical patients, mean differences in these outcomes were 6.4 days (p<0.0001), $21,448 (p<0.0001), and 14% (p<0.0001), respectively.</p><p><strong>Conclusion: </strong>Emergency care in patients with a higher co-morbid burden is more likely to lead to unplanned ICU admission, putting patients at a significantly increased chance of mortality, longer length of stay, and increased costs. Improving care and monitoring of patients outside the ICU may help detect early changes in pathophysiology and enable early intervention.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"15 \",\"pages\":\"703-719\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/ac/ceor-15-703.PMC10541084.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S424759\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S424759","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Patient Characteristics and Clinical and Economic Outcomes Associated with Unplanned Medical and Surgical Intensive Care Unit Admissions: A Retrospective Analysis.
Purpose: To characterize medical and surgical patient characteristics, as well as clinical and economic outcomes, associated with unplanned intensive care unit (ICU) admissions.
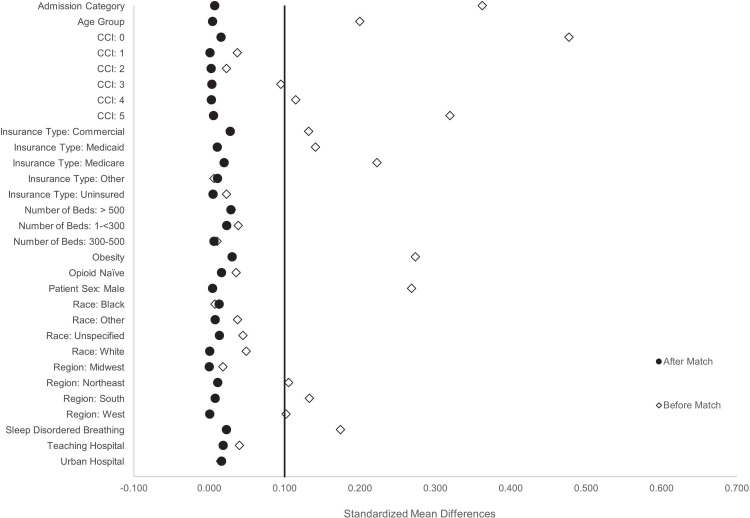
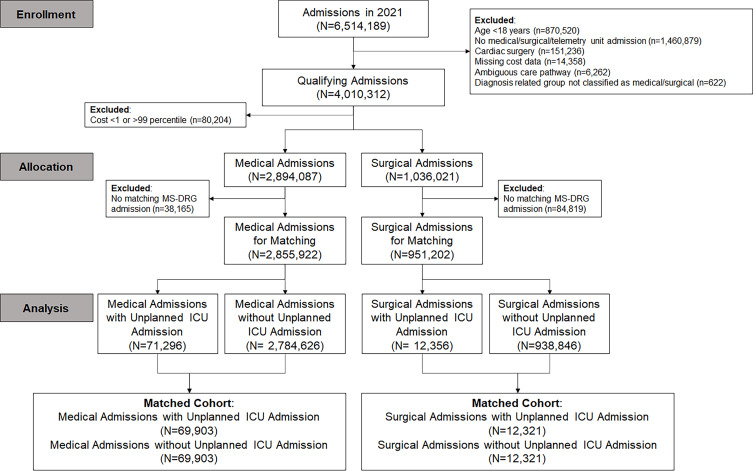
Patients and methods: This was a retrospective matched cohort analysis that utilized the PINC AITM Healthcare Database, which collects deidentified data from 25% of United States (US) hospital admissions. Discharge records were assessed for medical and surgical admissions in 2021. An unplanned ICU admission was defined as direct transfer from a medical, surgical, or telemetry unit to the ICU. Patients with and without an unplanned ICU admission were 1:1 propensity score matched. Differences between patients with and without unplanned ICU admissions were assessed using two-sample t-tests for continuous measures and Chi-square tests for categorical measures.
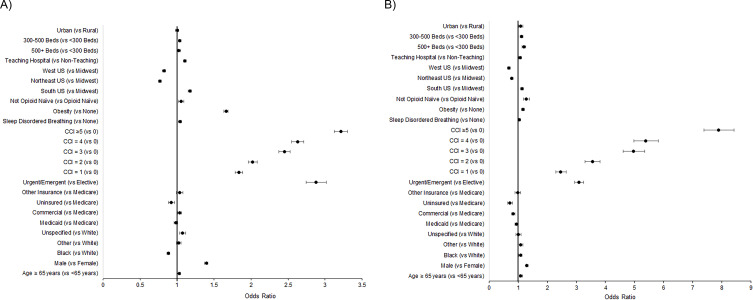
Results: A total of 3,807,124 qualifying admissions were identified. Medical admissions with unplanned ICU transfers were more likely to be urgent/emergent (odds ratio [OR] 2.9, 95% confidence interval [CI 2.7-3.0], p<0.0001), with patient characteristics including male sex (1.4, [1.4-1.4], p<0.0001), obesity (1.7, [1.6-1.7], p<0.0001), and increased Charlson Comorbidity Index (CCI=1: 1.8, [1.8-1.9], p<0.0001; CCI≥5: 3.2, [3.1-3.3], p<0.0001). Surgical admissions with unplanned ICU transfers were more likely to be urgent/emergent (3.1, [2.9-3.2], p<0.0001) and with patients of higher CCI (2.5, [2.3-2.6], p<0.0001 to a CCI of≥5 (7.9, [7.4-8.4], p<0.0001). Between matched medical patients, mean differences in length of stay, cost, and mortality were 4.1 days (p<0.0001), $13,424 (p<0.0001), and 21% (p<0.0001), respectively. Between matched surgical patients, mean differences in these outcomes were 6.4 days (p<0.0001), $21,448 (p<0.0001), and 14% (p<0.0001), respectively.
Conclusion: Emergency care in patients with a higher co-morbid burden is more likely to lead to unplanned ICU admission, putting patients at a significantly increased chance of mortality, longer length of stay, and increased costs. Improving care and monitoring of patients outside the ICU may help detect early changes in pathophysiology and enable early intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


