{"title":"澳大利亚悉尼德尔塔变异株流行期间四家医院爆发的医护人员严重急性呼吸系统综合征冠状病毒2型感染。","authors":"Danielle Hutchinson, Mohana Kunasekaran, Haley Stone, Xin Chen, Ashley Quigley, Aye Moa, C Raina MacIntyre","doi":"10.1155/2023/1806909","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Healthcare workers (HCWs) are at risk of SARS-CoV-2 infections due to occupational exposure. The use of airborne personal protective equipment (PPE) significantly reduces this risk. In June 2021, an epidemic of the Delta variant began in New South Wales (NSW), Australia. Concurrent PPE guidelines, set by the Clinical Excellence Commission (CEC), restricted the use of respirators.</p><p><strong>Objective: </strong>To understand the relationship of PPE guidelines with workplace-acquired HCW SARS-CoV-2 infections in different clinical settings and to examine the relationship between rates of community transmission and workplace-acquired HCW infections during the Delta outbreak in NSW.</p><p><strong>Methods: </strong>Total SARS-CoV-2 HCW infections between 13 June and 30 October 2021 (first four months of the Delta wave) were estimated from the government COVID-19 surveillance reports and compared with the surveillance reports of community transmission. In the absence of a detailed reporting of HCW infections, open-source data including news articles, media releases, and epidemiological surveillance reports were also collected. Data were extracted on HCW cases of SARS-CoV-2 from four hospitals, including the number of HCW cases (per NSW Health definition), clinical setting, PPE guidelines, and evidence of increasing local transmission.</p><p><strong>Results: </strong>SARS-CoV-2 infections in HCW identified as workplace-acquired infections (<i>n</i> = 177) and those without a known transmission source (<i>n</i> = 532) increased during the period of increasing community transmission (<i>n</i> = 75,014) in NSW. Four hospital COVID-19 clusters affecting 20 HCWs were identified between June and October 2021. HCW clusters occurred in general wards where staff were recommended to wear surgical masks. No workplace-acquired HCW infections were reported in these hospitals from critical care wards, where respirators were recommended during the same outbreak weeks.</p><p><strong>Conclusions: </strong>Differences in PPE policy across different wards may leave healthcare staff at risk of SARS-CoV-2 infection. During periods of high community transmission, respirators should be provided to protect hospital staff. Formal reporting of HCW infections should occur.</p>","PeriodicalId":46917,"journal":{"name":"Nursing Research and Practice","volume":"2023 ","pages":"1806909"},"PeriodicalIF":2.3000,"publicationDate":"2023-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10513866/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare Workers' SARS-CoV-2 Infections in Four Hospital Outbreaks during Delta Variant Prevalence in Sydney, Australia.\",\"authors\":\"Danielle Hutchinson, Mohana Kunasekaran, Haley Stone, Xin Chen, Ashley Quigley, Aye Moa, C Raina MacIntyre\",\"doi\":\"10.1155/2023/1806909\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Healthcare workers (HCWs) are at risk of SARS-CoV-2 infections due to occupational exposure. The use of airborne personal protective equipment (PPE) significantly reduces this risk. In June 2021, an epidemic of the Delta variant began in New South Wales (NSW), Australia. Concurrent PPE guidelines, set by the Clinical Excellence Commission (CEC), restricted the use of respirators.</p><p><strong>Objective: </strong>To understand the relationship of PPE guidelines with workplace-acquired HCW SARS-CoV-2 infections in different clinical settings and to examine the relationship between rates of community transmission and workplace-acquired HCW infections during the Delta outbreak in NSW.</p><p><strong>Methods: </strong>Total SARS-CoV-2 HCW infections between 13 June and 30 October 2021 (first four months of the Delta wave) were estimated from the government COVID-19 surveillance reports and compared with the surveillance reports of community transmission. In the absence of a detailed reporting of HCW infections, open-source data including news articles, media releases, and epidemiological surveillance reports were also collected. Data were extracted on HCW cases of SARS-CoV-2 from four hospitals, including the number of HCW cases (per NSW Health definition), clinical setting, PPE guidelines, and evidence of increasing local transmission.</p><p><strong>Results: </strong>SARS-CoV-2 infections in HCW identified as workplace-acquired infections (<i>n</i> = 177) and those without a known transmission source (<i>n</i> = 532) increased during the period of increasing community transmission (<i>n</i> = 75,014) in NSW. Four hospital COVID-19 clusters affecting 20 HCWs were identified between June and October 2021. HCW clusters occurred in general wards where staff were recommended to wear surgical masks. No workplace-acquired HCW infections were reported in these hospitals from critical care wards, where respirators were recommended during the same outbreak weeks.</p><p><strong>Conclusions: </strong>Differences in PPE policy across different wards may leave healthcare staff at risk of SARS-CoV-2 infection. During periods of high community transmission, respirators should be provided to protect hospital staff. Formal reporting of HCW infections should occur.</p>\",\"PeriodicalId\":46917,\"journal\":{\"name\":\"Nursing Research and Practice\",\"volume\":\"2023 \",\"pages\":\"1806909\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-09-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10513866/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nursing Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/1806909\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"NURSING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nursing Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/1806909","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"NURSING","Score":null,"Total":0}
Healthcare Workers' SARS-CoV-2 Infections in Four Hospital Outbreaks during Delta Variant Prevalence in Sydney, Australia.
Background: Healthcare workers (HCWs) are at risk of SARS-CoV-2 infections due to occupational exposure. The use of airborne personal protective equipment (PPE) significantly reduces this risk. In June 2021, an epidemic of the Delta variant began in New South Wales (NSW), Australia. Concurrent PPE guidelines, set by the Clinical Excellence Commission (CEC), restricted the use of respirators.
Objective: To understand the relationship of PPE guidelines with workplace-acquired HCW SARS-CoV-2 infections in different clinical settings and to examine the relationship between rates of community transmission and workplace-acquired HCW infections during the Delta outbreak in NSW.
Methods: Total SARS-CoV-2 HCW infections between 13 June and 30 October 2021 (first four months of the Delta wave) were estimated from the government COVID-19 surveillance reports and compared with the surveillance reports of community transmission. In the absence of a detailed reporting of HCW infections, open-source data including news articles, media releases, and epidemiological surveillance reports were also collected. Data were extracted on HCW cases of SARS-CoV-2 from four hospitals, including the number of HCW cases (per NSW Health definition), clinical setting, PPE guidelines, and evidence of increasing local transmission.
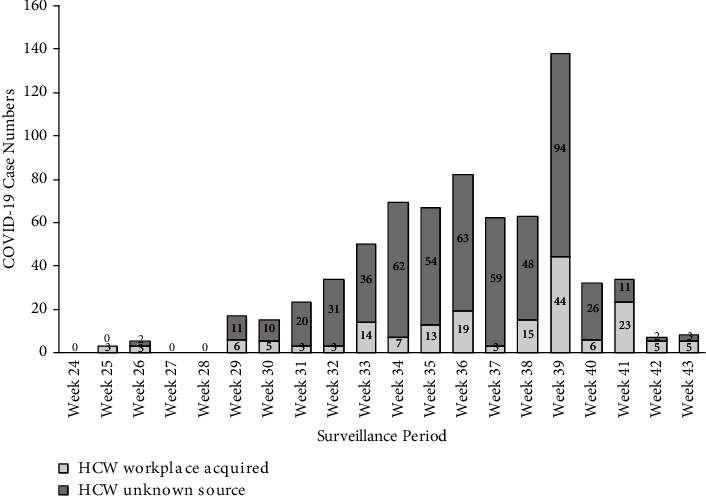
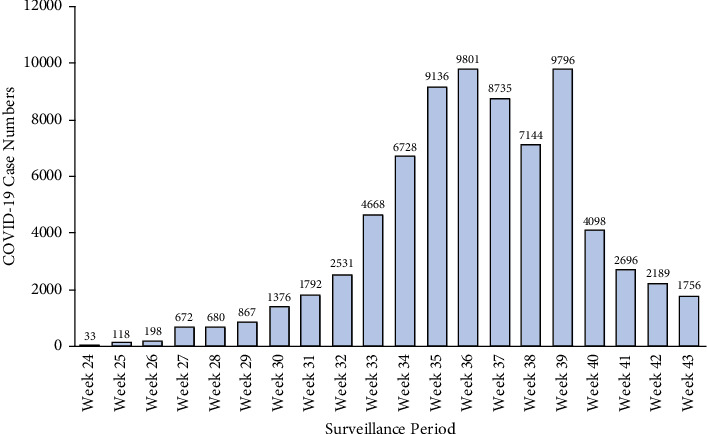
Results: SARS-CoV-2 infections in HCW identified as workplace-acquired infections (n = 177) and those without a known transmission source (n = 532) increased during the period of increasing community transmission (n = 75,014) in NSW. Four hospital COVID-19 clusters affecting 20 HCWs were identified between June and October 2021. HCW clusters occurred in general wards where staff were recommended to wear surgical masks. No workplace-acquired HCW infections were reported in these hospitals from critical care wards, where respirators were recommended during the same outbreak weeks.
Conclusions: Differences in PPE policy across different wards may leave healthcare staff at risk of SARS-CoV-2 infection. During periods of high community transmission, respirators should be provided to protect hospital staff. Formal reporting of HCW infections should occur.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


