Caroline Hedsund, Kasper Linde Ankjærgaard, Tine Peick Sonne, Philip Tønnesen, Ejvind Frausing Hansen, Helle Frost Andreassen, Ronan M G Berg, Jens-Ulrik Stæhr Jensen, Jon Torgny Wilcke
{"title":"COPD患者急性高碳酸血症呼吸衰竭加重后的长期无创通气:一项随机对照试验。","authors":"Caroline Hedsund, Kasper Linde Ankjærgaard, Tine Peick Sonne, Philip Tønnesen, Ejvind Frausing Hansen, Helle Frost Andreassen, Ronan M G Berg, Jens-Ulrik Stæhr Jensen, Jon Torgny Wilcke","doi":"10.1080/20018525.2023.2257993","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>It remains unclear whether long-term non-invasive ventilation (LT-NIV) for patients with chronic obstructive pulmonary disease (COPD) improves survival and reduces admissions as results from randomized trials are inconsistent. We aim to determine whether LT-NIV initiated after an admission with acute hypercapnic respiratory failure (AHRF) can affect survival and admission rate in COPD patients.</p><p><strong>Methods: </strong>A randomized controlled open-label trial, allocating patients with COPD to LT-NIV or standard of care immediately after an admission with AHRF treated with acute NIV. LT-NIV was aimed to normalize PaCO<sub>2</sub> using high-pressure NIV.</p><p><strong>Results: </strong>The study was discontinued before full sample size due to slow recruitment. 28 patients were randomized to LT-NIV and 27 patients to standard of care. 42% of patients had a history of ≥ 2 admissions with AHRF. Median IPAP was 24 cmH<sub>2</sub>O (IQR 20-28). The primary outcome, time to readmission with AHRF or death within 12 months, did not reach significance, hazard ratio 0.53 (95% CI 0.25-1.12) <i>p</i> = 0.097. In a competing risk analysis, adjusted for history of AHRF, the odds ratio for AHRF within 12 months was 0.30 (95% CI 0.11-0.87) <i>p</i> = 0.024. The LT-NIV group had less exacerbations (median 1 (0-1) vs 2 (1-4) <i>p</i> = 0.021) and readmissions with AHRF (median 0 (0-1) vs 1 (0-1) <i>p</i> = 0.016).</p><p><strong>Conclusion: </strong>The risk of the primary outcome, time to readmission with AHRF or death within 12 months was numerically smaller in the LT-NIV group, however, did not reach significance. Nevertheless, several secondary outcome analyses like risk of AHRF, number of episodes of AHRF and exacerbations were all significantly reduced in favour of high-pressure LT-NIV, especially in patients with frequent AHRF.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"10 1","pages":"2257993"},"PeriodicalIF":1.4000,"publicationDate":"2023-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/85/02/ZECR_10_2257993.PMC10512815.pdf","citationCount":"0","resultStr":"{\"title\":\"Long-term non-invasive ventilation for COPD patients following an exacerbation with acute hypercapnic respiratory failure: a randomized controlled trial.\",\"authors\":\"Caroline Hedsund, Kasper Linde Ankjærgaard, Tine Peick Sonne, Philip Tønnesen, Ejvind Frausing Hansen, Helle Frost Andreassen, Ronan M G Berg, Jens-Ulrik Stæhr Jensen, Jon Torgny Wilcke\",\"doi\":\"10.1080/20018525.2023.2257993\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>It remains unclear whether long-term non-invasive ventilation (LT-NIV) for patients with chronic obstructive pulmonary disease (COPD) improves survival and reduces admissions as results from randomized trials are inconsistent. We aim to determine whether LT-NIV initiated after an admission with acute hypercapnic respiratory failure (AHRF) can affect survival and admission rate in COPD patients.</p><p><strong>Methods: </strong>A randomized controlled open-label trial, allocating patients with COPD to LT-NIV or standard of care immediately after an admission with AHRF treated with acute NIV. LT-NIV was aimed to normalize PaCO<sub>2</sub> using high-pressure NIV.</p><p><strong>Results: </strong>The study was discontinued before full sample size due to slow recruitment. 28 patients were randomized to LT-NIV and 27 patients to standard of care. 42% of patients had a history of ≥ 2 admissions with AHRF. Median IPAP was 24 cmH<sub>2</sub>O (IQR 20-28). The primary outcome, time to readmission with AHRF or death within 12 months, did not reach significance, hazard ratio 0.53 (95% CI 0.25-1.12) <i>p</i> = 0.097. In a competing risk analysis, adjusted for history of AHRF, the odds ratio for AHRF within 12 months was 0.30 (95% CI 0.11-0.87) <i>p</i> = 0.024. The LT-NIV group had less exacerbations (median 1 (0-1) vs 2 (1-4) <i>p</i> = 0.021) and readmissions with AHRF (median 0 (0-1) vs 1 (0-1) <i>p</i> = 0.016).</p><p><strong>Conclusion: </strong>The risk of the primary outcome, time to readmission with AHRF or death within 12 months was numerically smaller in the LT-NIV group, however, did not reach significance. Nevertheless, several secondary outcome analyses like risk of AHRF, number of episodes of AHRF and exacerbations were all significantly reduced in favour of high-pressure LT-NIV, especially in patients with frequent AHRF.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"10 1\",\"pages\":\"2257993\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/85/02/ZECR_10_2257993.PMC10512815.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2023.2257993\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2023.2257993","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Long-term non-invasive ventilation for COPD patients following an exacerbation with acute hypercapnic respiratory failure: a randomized controlled trial.
Introduction: It remains unclear whether long-term non-invasive ventilation (LT-NIV) for patients with chronic obstructive pulmonary disease (COPD) improves survival and reduces admissions as results from randomized trials are inconsistent. We aim to determine whether LT-NIV initiated after an admission with acute hypercapnic respiratory failure (AHRF) can affect survival and admission rate in COPD patients.
Methods: A randomized controlled open-label trial, allocating patients with COPD to LT-NIV or standard of care immediately after an admission with AHRF treated with acute NIV. LT-NIV was aimed to normalize PaCO2 using high-pressure NIV.
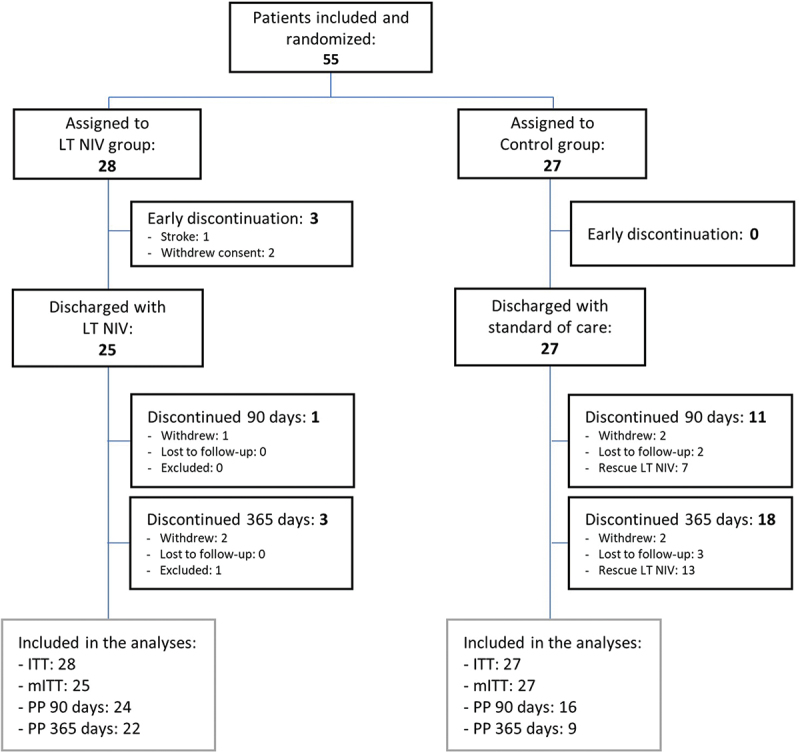
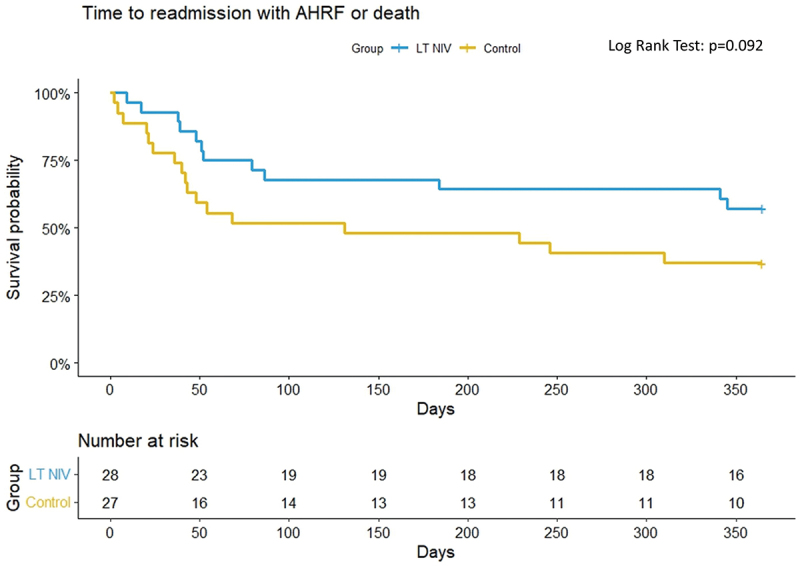
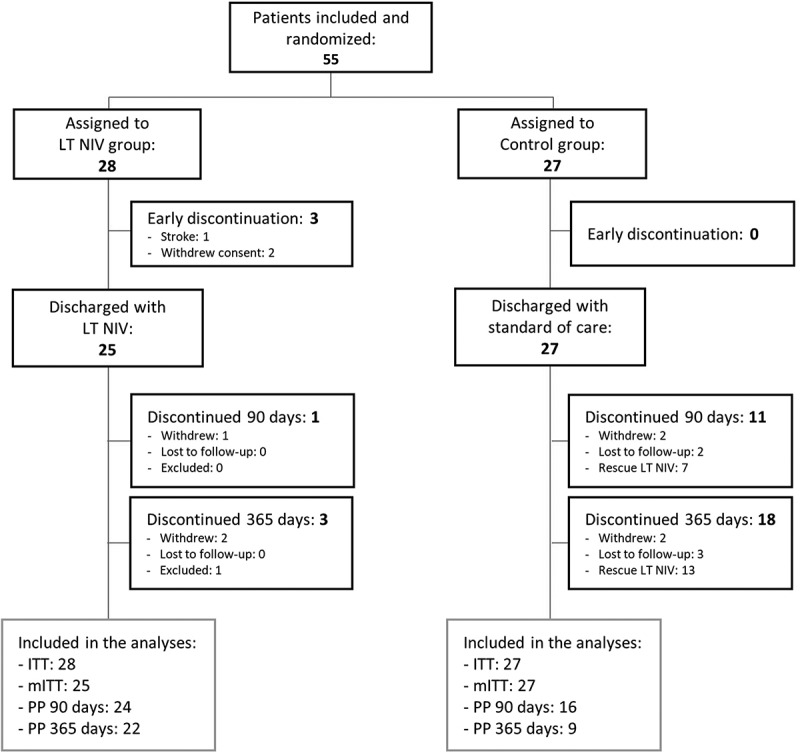
Results: The study was discontinued before full sample size due to slow recruitment. 28 patients were randomized to LT-NIV and 27 patients to standard of care. 42% of patients had a history of ≥ 2 admissions with AHRF. Median IPAP was 24 cmH2O (IQR 20-28). The primary outcome, time to readmission with AHRF or death within 12 months, did not reach significance, hazard ratio 0.53 (95% CI 0.25-1.12) p = 0.097. In a competing risk analysis, adjusted for history of AHRF, the odds ratio for AHRF within 12 months was 0.30 (95% CI 0.11-0.87) p = 0.024. The LT-NIV group had less exacerbations (median 1 (0-1) vs 2 (1-4) p = 0.021) and readmissions with AHRF (median 0 (0-1) vs 1 (0-1) p = 0.016).
Conclusion: The risk of the primary outcome, time to readmission with AHRF or death within 12 months was numerically smaller in the LT-NIV group, however, did not reach significance. Nevertheless, several secondary outcome analyses like risk of AHRF, number of episodes of AHRF and exacerbations were all significantly reduced in favour of high-pressure LT-NIV, especially in patients with frequent AHRF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


