{"title":"免疫组织化学PD-L1检测指导的NSCLC患者免疫治疗:基于微刺激模型的有效性和成本效益分析。","authors":"Mingjun Rui, Yingcheng Wang, Yunfei Li, Zhengyang Fei","doi":"10.1007/s40259-023-00628-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>On the basis of immunohistochemistry PD-L1 testing results, patients with advanced non-small cell lung cancer (NSCLC) are treated differently. Theoretically, patients with high PD-L1 expression (50% or 1%) should receive PD-1 monotherapy for fewer adverse reactions and cost savings from avoiding chemotherapy; however, there is controversy surrounding the cut-off criteria (1% or 50%) for immunohistochemistry testing and threshold for PD-1 monotherapy.</p><p><strong>Objective: </strong>This study aims to predict the effectiveness and cost-effectiveness of different immunotherapy strategies for patients with NSCLC in China from the healthcare system perspective.</p><p><strong>Patients and methods: </strong>A microsimulation model was developed to evaluate the effectiveness and cost-effectiveness of three treatment strategies: PD-L1 testing (1%) (PD-1 monotherapy for those with PD-L1 expression at 1% threshold, and combination with chemotherapy for others with immunohistochemistry testing), PD-L1 testing (50%) (PD-1 monotherapy for those with PD-L1 expression at 50% threshold, and combination with chemotherapy for others with immunohistochemistry testing), and No PD-L1 testing (PD-1 combined with chemotherapy without immunohistochemistry testing). The model assumed 1000 patients per strategy, with each patient entering a unique clinical path prior to receiving treatment on the basis of PD-L1 test results. Clinical inputs were derived from clinical trials. Cost and utility parameters were obtained from the database and literature. One-way probabilistic sensitivity analyses (PSA) and six scenario analyses were used to test the model's robustness.</p><p><strong>Results: </strong>The study revealed a hierarchy of survival benefits across three strategies, with No PD-L1 testing demonstrating the most survival advantage, followed by PD-L1 testing (50%), and finally, PD-L1 testing (1%). The comparative analysis demonstrated that No PD-L1 testing significantly enhanced overall survival (OS) (HR 0.85, 95% CI 0.78-0.93), progression-free survival (HR 0.82, 95% CI 0.75-0.90), and progression-free2 survival (PFS2) (HR 0.91, 95% CI 0.83-0.99) when juxtaposed against PD-L1 testing (1%). However, these improvements were not as pronounced when compared with PD-L1 testing (50%), particularly in relation to PFS, PFS2, and OS. The cost-effectiveness analysis further unveiled incremental cost-utility ratios (ICUR), with No PD-L1 testing versus PD-L1 testing (50%) at $34,003 per quality-adjusted life year (QALY) and No PD-L1 testing versus PD-L1 testing (1%) at $34,804 per QALY. In parallel, the ICUR for PD-L1 testing (50%) versus PD-L1 testing (1%) stood at $35,713 per QALY. Remarkably, the PSA result under a willingness-to-pay (WTP) threshold of $10,144 per QALY, with a 100% probability, demonstrated PD-L1 testing (1%) as the most cost-effective option.</p><p><strong>Conclusions: </strong>The survival benefits of PD-1 monotherapy for high expression with PD-L1 immunohistochemistry testing are inferior to those of PD-1 combined with chemotherapy without testing, but it is found to be more cost-effective at the WTP thresholds in China and holds great potential in increasing affordability and reducing the economic burden.</p>","PeriodicalId":9022,"journal":{"name":"BioDrugs","volume":" ","pages":"157-170"},"PeriodicalIF":5.4000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Immunotherapy Guided by Immunohistochemistry PD-L1 Testing for Patients with NSCLC: A Microsimulation Model-Based Effectiveness and Cost-Effectiveness Analysis.\",\"authors\":\"Mingjun Rui, Yingcheng Wang, Yunfei Li, Zhengyang Fei\",\"doi\":\"10.1007/s40259-023-00628-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>On the basis of immunohistochemistry PD-L1 testing results, patients with advanced non-small cell lung cancer (NSCLC) are treated differently. Theoretically, patients with high PD-L1 expression (50% or 1%) should receive PD-1 monotherapy for fewer adverse reactions and cost savings from avoiding chemotherapy; however, there is controversy surrounding the cut-off criteria (1% or 50%) for immunohistochemistry testing and threshold for PD-1 monotherapy.</p><p><strong>Objective: </strong>This study aims to predict the effectiveness and cost-effectiveness of different immunotherapy strategies for patients with NSCLC in China from the healthcare system perspective.</p><p><strong>Patients and methods: </strong>A microsimulation model was developed to evaluate the effectiveness and cost-effectiveness of three treatment strategies: PD-L1 testing (1%) (PD-1 monotherapy for those with PD-L1 expression at 1% threshold, and combination with chemotherapy for others with immunohistochemistry testing), PD-L1 testing (50%) (PD-1 monotherapy for those with PD-L1 expression at 50% threshold, and combination with chemotherapy for others with immunohistochemistry testing), and No PD-L1 testing (PD-1 combined with chemotherapy without immunohistochemistry testing). The model assumed 1000 patients per strategy, with each patient entering a unique clinical path prior to receiving treatment on the basis of PD-L1 test results. Clinical inputs were derived from clinical trials. Cost and utility parameters were obtained from the database and literature. One-way probabilistic sensitivity analyses (PSA) and six scenario analyses were used to test the model's robustness.</p><p><strong>Results: </strong>The study revealed a hierarchy of survival benefits across three strategies, with No PD-L1 testing demonstrating the most survival advantage, followed by PD-L1 testing (50%), and finally, PD-L1 testing (1%). The comparative analysis demonstrated that No PD-L1 testing significantly enhanced overall survival (OS) (HR 0.85, 95% CI 0.78-0.93), progression-free survival (HR 0.82, 95% CI 0.75-0.90), and progression-free2 survival (PFS2) (HR 0.91, 95% CI 0.83-0.99) when juxtaposed against PD-L1 testing (1%). However, these improvements were not as pronounced when compared with PD-L1 testing (50%), particularly in relation to PFS, PFS2, and OS. The cost-effectiveness analysis further unveiled incremental cost-utility ratios (ICUR), with No PD-L1 testing versus PD-L1 testing (50%) at $34,003 per quality-adjusted life year (QALY) and No PD-L1 testing versus PD-L1 testing (1%) at $34,804 per QALY. In parallel, the ICUR for PD-L1 testing (50%) versus PD-L1 testing (1%) stood at $35,713 per QALY. Remarkably, the PSA result under a willingness-to-pay (WTP) threshold of $10,144 per QALY, with a 100% probability, demonstrated PD-L1 testing (1%) as the most cost-effective option.</p><p><strong>Conclusions: </strong>The survival benefits of PD-1 monotherapy for high expression with PD-L1 immunohistochemistry testing are inferior to those of PD-1 combined with chemotherapy without testing, but it is found to be more cost-effective at the WTP thresholds in China and holds great potential in increasing affordability and reducing the economic burden.</p>\",\"PeriodicalId\":9022,\"journal\":{\"name\":\"BioDrugs\",\"volume\":\" \",\"pages\":\"157-170\"},\"PeriodicalIF\":5.4000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BioDrugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40259-023-00628-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BioDrugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40259-023-00628-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Immunotherapy Guided by Immunohistochemistry PD-L1 Testing for Patients with NSCLC: A Microsimulation Model-Based Effectiveness and Cost-Effectiveness Analysis.
Background: On the basis of immunohistochemistry PD-L1 testing results, patients with advanced non-small cell lung cancer (NSCLC) are treated differently. Theoretically, patients with high PD-L1 expression (50% or 1%) should receive PD-1 monotherapy for fewer adverse reactions and cost savings from avoiding chemotherapy; however, there is controversy surrounding the cut-off criteria (1% or 50%) for immunohistochemistry testing and threshold for PD-1 monotherapy.
Objective: This study aims to predict the effectiveness and cost-effectiveness of different immunotherapy strategies for patients with NSCLC in China from the healthcare system perspective.
Patients and methods: A microsimulation model was developed to evaluate the effectiveness and cost-effectiveness of three treatment strategies: PD-L1 testing (1%) (PD-1 monotherapy for those with PD-L1 expression at 1% threshold, and combination with chemotherapy for others with immunohistochemistry testing), PD-L1 testing (50%) (PD-1 monotherapy for those with PD-L1 expression at 50% threshold, and combination with chemotherapy for others with immunohistochemistry testing), and No PD-L1 testing (PD-1 combined with chemotherapy without immunohistochemistry testing). The model assumed 1000 patients per strategy, with each patient entering a unique clinical path prior to receiving treatment on the basis of PD-L1 test results. Clinical inputs were derived from clinical trials. Cost and utility parameters were obtained from the database and literature. One-way probabilistic sensitivity analyses (PSA) and six scenario analyses were used to test the model's robustness.
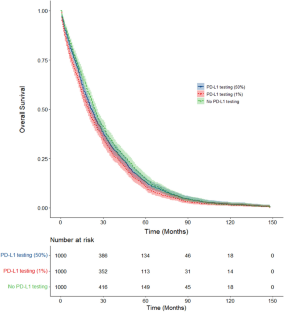
Results: The study revealed a hierarchy of survival benefits across three strategies, with No PD-L1 testing demonstrating the most survival advantage, followed by PD-L1 testing (50%), and finally, PD-L1 testing (1%). The comparative analysis demonstrated that No PD-L1 testing significantly enhanced overall survival (OS) (HR 0.85, 95% CI 0.78-0.93), progression-free survival (HR 0.82, 95% CI 0.75-0.90), and progression-free2 survival (PFS2) (HR 0.91, 95% CI 0.83-0.99) when juxtaposed against PD-L1 testing (1%). However, these improvements were not as pronounced when compared with PD-L1 testing (50%), particularly in relation to PFS, PFS2, and OS. The cost-effectiveness analysis further unveiled incremental cost-utility ratios (ICUR), with No PD-L1 testing versus PD-L1 testing (50%) at $34,003 per quality-adjusted life year (QALY) and No PD-L1 testing versus PD-L1 testing (1%) at $34,804 per QALY. In parallel, the ICUR for PD-L1 testing (50%) versus PD-L1 testing (1%) stood at $35,713 per QALY. Remarkably, the PSA result under a willingness-to-pay (WTP) threshold of $10,144 per QALY, with a 100% probability, demonstrated PD-L1 testing (1%) as the most cost-effective option.
Conclusions: The survival benefits of PD-1 monotherapy for high expression with PD-L1 immunohistochemistry testing are inferior to those of PD-1 combined with chemotherapy without testing, but it is found to be more cost-effective at the WTP thresholds in China and holds great potential in increasing affordability and reducing the economic burden.
期刊介绍:
An essential resource for R&D professionals and clinicians with an interest in biologic therapies.
BioDrugs covers the development and therapeutic application of biotechnology-based pharmaceuticals and diagnostic products for the treatment of human disease.
BioDrugs offers a range of additional enhanced features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist patients, caregivers and others in understanding important medical advances. The journal also provides the option to include various other types of enhanced features including slide sets, videos and animations. All enhanced features are peer reviewed to the same high standard as the article itself. Peer review is conducted using Editorial Manager®, supported by a database of international experts. This database is shared with other Adis journals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


