{"title":"弥漫大 B 细胞淋巴瘤老年患者的口服化疗应用:回顾性分析中的替代方案","authors":"Pi-Han Liao, Ching-Yuan Kuo, Ming-Chun Ma, Chin-Kai Liao, Sung-Nan Pei, Ming-Chung Wang","doi":"10.14740/jh1054","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered the standard treatment for diffuse large B-cell lymphoma (DLBCL). However, no standard treatment has been established for older patients (age ≥ 75 years). This study retrospectively analyzed different treatment strategies in older patients with DLBCL with different chemotherapy regimens and compared the survival rate of patients using oral or intravenous form cyclophosphamide and etoposide in a single center.</p><p><strong>Methods: </strong>We reviewed the records of older patients with DLBCL, aged ≥ 75 years, from January 2010 to August 2019. The different treatment combinations, clinical characteristics, response rates, and toxicity profiles were analyzed. The median overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier (KM) method. Cox regression model was used to identify the risk factors.</p><p><strong>Results: </strong>Eighty-four patients were included. One-quarter of the patients received cytoreduction treatment because of their poor medical condition at the time of diagnosis. Twenty-six percent of the patients were aged ≥ 85 at the time of diagnosis and 46.7% completed the treatment course. Patients receiving non-anthracycline-containing (non-ACR) treatment had worse Charlson comorbidity index, worse PFS, lower body mass index, or were older. The mean anthracycline accumulative dose in the anthracycline-containing (ACR) group was 134 mg/m<sup>2</sup>. The median OS was 17.2 months and median PFS was 7.7 months. The PFS of R-CHOP is better than R-mini-CHOP and R-CVOP without statistical significance, but OS of R-CHOP is not better than the other regimens.</p><p><strong>Conclusion: </strong>The toxicity, efficacy, and KM curve for OS and PFS in the non-ACR group were lower compared to ACR group, without statistical significance. R-CVOP had similar OS with R-mini-CHOP in our study. The result does not mean etoposide could totally substitute for anthracycline, but etoposide did have lower early progression rate (12.5%), and it may be an option for frail patients with comorbidity. Oral form cyclophosphamide and etoposide could be considered as a substitute for intravenous administration because of the similar effect and toxic profile.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"11 5","pages":"176-184"},"PeriodicalIF":1.3000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/64/7e/jh-11-176.PMC9635798.pdf","citationCount":"0","resultStr":"{\"title\":\"Oral Chemotherapy Application in Elderly Patients With Diffuse Large B-Cell Lymphoma: An Alternative Regimen in Retrospective Analysis.\",\"authors\":\"Pi-Han Liao, Ching-Yuan Kuo, Ming-Chun Ma, Chin-Kai Liao, Sung-Nan Pei, Ming-Chung Wang\",\"doi\":\"10.14740/jh1054\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered the standard treatment for diffuse large B-cell lymphoma (DLBCL). However, no standard treatment has been established for older patients (age ≥ 75 years). This study retrospectively analyzed different treatment strategies in older patients with DLBCL with different chemotherapy regimens and compared the survival rate of patients using oral or intravenous form cyclophosphamide and etoposide in a single center.</p><p><strong>Methods: </strong>We reviewed the records of older patients with DLBCL, aged ≥ 75 years, from January 2010 to August 2019. The different treatment combinations, clinical characteristics, response rates, and toxicity profiles were analyzed. The median overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier (KM) method. Cox regression model was used to identify the risk factors.</p><p><strong>Results: </strong>Eighty-four patients were included. One-quarter of the patients received cytoreduction treatment because of their poor medical condition at the time of diagnosis. Twenty-six percent of the patients were aged ≥ 85 at the time of diagnosis and 46.7% completed the treatment course. Patients receiving non-anthracycline-containing (non-ACR) treatment had worse Charlson comorbidity index, worse PFS, lower body mass index, or were older. The mean anthracycline accumulative dose in the anthracycline-containing (ACR) group was 134 mg/m<sup>2</sup>. The median OS was 17.2 months and median PFS was 7.7 months. The PFS of R-CHOP is better than R-mini-CHOP and R-CVOP without statistical significance, but OS of R-CHOP is not better than the other regimens.</p><p><strong>Conclusion: </strong>The toxicity, efficacy, and KM curve for OS and PFS in the non-ACR group were lower compared to ACR group, without statistical significance. R-CVOP had similar OS with R-mini-CHOP in our study. The result does not mean etoposide could totally substitute for anthracycline, but etoposide did have lower early progression rate (12.5%), and it may be an option for frail patients with comorbidity. Oral form cyclophosphamide and etoposide could be considered as a substitute for intravenous administration because of the similar effect and toxic profile.</p>\",\"PeriodicalId\":15964,\"journal\":{\"name\":\"Journal of hematology\",\"volume\":\"11 5\",\"pages\":\"176-184\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/64/7e/jh-11-176.PMC9635798.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jh1054\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/31 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:利妥昔单抗、环磷酰胺、多柔比星、长春新碱和泼尼松(R-CHOP)联合疗法被认为是弥漫大 B 细胞淋巴瘤(DLBCL)的标准疗法。然而,老年患者(年龄≥ 75 岁)的标准治疗方法尚未确立。本研究回顾性分析了老年DLBCL患者采用不同化疗方案的不同治疗策略,并比较了在一个中心使用口服或静脉注射环磷酰胺和依托泊苷的患者的生存率:我们回顾了2010年1月至2019年8月年龄≥75岁的DLBCL老年患者的病历。分析了不同的治疗组合、临床特征、反应率和毒性概况。采用卡普兰-梅耶(KM)法估算了中位总生存期(OS)和无进展生存期(PFS)。采用Cox回归模型确定风险因素:结果:共纳入84例患者。四分之一的患者因确诊时身体状况较差而接受了细胞减灭术治疗。26%的患者确诊时年龄≥85岁,46.7%的患者完成了疗程。接受不含蒽环类药物(非蒽环类药物)治疗的患者夏尔森合并症指数较低,PFS较差,体重指数较低或年龄较大。含蒽环类药物(ACR)组的平均蒽环类药物累积剂量为134毫克/平方米。中位OS为17.2个月,中位PFS为7.7个月。R-CHOP的PFS优于R-迷你CHOP和R-CVOP,但无统计学意义,但R-CHOP的OS不优于其他方案:结论:非 ACR 组的毒性、疗效以及 OS 和 PFS 的 KM 曲线均低于 ACR 组,但无统计学意义。在我们的研究中,R-CVOP 与 R-mini-CHOP 的 OS 相似。这一结果并不意味着依托泊苷可以完全替代蒽环类药物,但依托泊苷的早期进展率确实较低(12.5%),对于有合并症的体弱患者来说,依托泊苷可能是一种选择。口服环磷酰胺和依托泊苷的疗效和毒性相似,因此可考虑用其替代静脉注射。
Oral Chemotherapy Application in Elderly Patients With Diffuse Large B-Cell Lymphoma: An Alternative Regimen in Retrospective Analysis.
Background: A combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered the standard treatment for diffuse large B-cell lymphoma (DLBCL). However, no standard treatment has been established for older patients (age ≥ 75 years). This study retrospectively analyzed different treatment strategies in older patients with DLBCL with different chemotherapy regimens and compared the survival rate of patients using oral or intravenous form cyclophosphamide and etoposide in a single center.
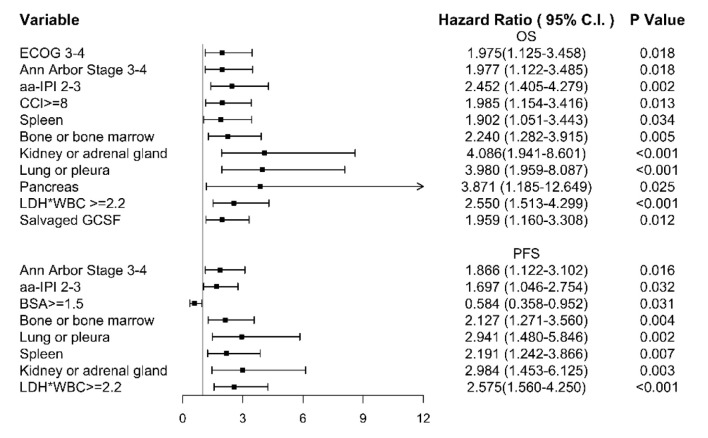
Methods: We reviewed the records of older patients with DLBCL, aged ≥ 75 years, from January 2010 to August 2019. The different treatment combinations, clinical characteristics, response rates, and toxicity profiles were analyzed. The median overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier (KM) method. Cox regression model was used to identify the risk factors.
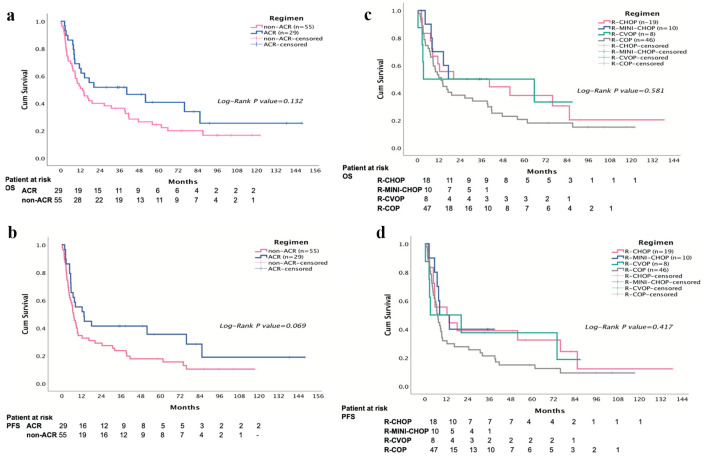
Results: Eighty-four patients were included. One-quarter of the patients received cytoreduction treatment because of their poor medical condition at the time of diagnosis. Twenty-six percent of the patients were aged ≥ 85 at the time of diagnosis and 46.7% completed the treatment course. Patients receiving non-anthracycline-containing (non-ACR) treatment had worse Charlson comorbidity index, worse PFS, lower body mass index, or were older. The mean anthracycline accumulative dose in the anthracycline-containing (ACR) group was 134 mg/m2. The median OS was 17.2 months and median PFS was 7.7 months. The PFS of R-CHOP is better than R-mini-CHOP and R-CVOP without statistical significance, but OS of R-CHOP is not better than the other regimens.
Conclusion: The toxicity, efficacy, and KM curve for OS and PFS in the non-ACR group were lower compared to ACR group, without statistical significance. R-CVOP had similar OS with R-mini-CHOP in our study. The result does not mean etoposide could totally substitute for anthracycline, but etoposide did have lower early progression rate (12.5%), and it may be an option for frail patients with comorbidity. Oral form cyclophosphamide and etoposide could be considered as a substitute for intravenous administration because of the similar effect and toxic profile.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


