Christian Schneider, Meike K Wassermann, Gereon R Fink, Helmar C Lehmann
{"title":"非全身性血管性神经病变诱导治疗的单中心经验。","authors":"Christian Schneider, Meike K Wassermann, Gereon R Fink, Helmar C Lehmann","doi":"10.1186/s42466-022-00198-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>No controlled studies for non-systemic vasculitic neuropathy treatment exist (NSVN). We compared the treatment response to induction therapy commonly used in clinical practice in NSVN.</p><p><strong>Methods: </strong>In this retrospective single-center study, 43 patients with biopsy-proven NSVN were analyzed. Patients were subdivided into groups depending on their initial treatment. Relapse rates, changes of motor and sensory symptoms, adverse events, predictors of relapses, and second-line treatment were compared.</p><p><strong>Results: </strong>Initial treatment regimens were corticosteroid monotherapy, cyclophosphamide monotherapy, pulsed corticosteroid therapy, and combination therapy. Discontinuation due to adverse events occurred in 6 of 43 patients. Clinical data did not differ between treatment groups. Within 12 months, 24.3% of patients relapsed. The median time to relapse was 4 (1.5, 6) months. No relapse occurred in the combination therapy group. However, there was no statistically significant difference in relapse-free survival between treatment groups (p = 0.58). Neither clinical data nor biopsy analysis predicted relapses sufficiently. As a second-line treatment, cyclophosphamide as mono- or combination therapy was used (7 of 9 patients) most frequently. One patient was treated with methotrexate, and one with IVIG.</p><p><strong>Conclusions: </strong>Induction therapy used in clinical practice is effective and mainly well-tolerated in NSVN. Our data do not support an overall advantage of cyclophosphamide over corticosteroid monotherapy. Controlled trials comparing the effectiveness of induction and maintenance therapy in NSVN are warranted.</p>","PeriodicalId":19169,"journal":{"name":"Neurological Research and Practice","volume":" ","pages":"32"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9377119/pdf/","citationCount":"1","resultStr":"{\"title\":\"Single-center experience of induction therapy in non-systemic vasculitic neuropathy.\",\"authors\":\"Christian Schneider, Meike K Wassermann, Gereon R Fink, Helmar C Lehmann\",\"doi\":\"10.1186/s42466-022-00198-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>No controlled studies for non-systemic vasculitic neuropathy treatment exist (NSVN). We compared the treatment response to induction therapy commonly used in clinical practice in NSVN.</p><p><strong>Methods: </strong>In this retrospective single-center study, 43 patients with biopsy-proven NSVN were analyzed. Patients were subdivided into groups depending on their initial treatment. Relapse rates, changes of motor and sensory symptoms, adverse events, predictors of relapses, and second-line treatment were compared.</p><p><strong>Results: </strong>Initial treatment regimens were corticosteroid monotherapy, cyclophosphamide monotherapy, pulsed corticosteroid therapy, and combination therapy. Discontinuation due to adverse events occurred in 6 of 43 patients. Clinical data did not differ between treatment groups. Within 12 months, 24.3% of patients relapsed. The median time to relapse was 4 (1.5, 6) months. No relapse occurred in the combination therapy group. However, there was no statistically significant difference in relapse-free survival between treatment groups (p = 0.58). Neither clinical data nor biopsy analysis predicted relapses sufficiently. As a second-line treatment, cyclophosphamide as mono- or combination therapy was used (7 of 9 patients) most frequently. One patient was treated with methotrexate, and one with IVIG.</p><p><strong>Conclusions: </strong>Induction therapy used in clinical practice is effective and mainly well-tolerated in NSVN. Our data do not support an overall advantage of cyclophosphamide over corticosteroid monotherapy. Controlled trials comparing the effectiveness of induction and maintenance therapy in NSVN are warranted.</p>\",\"PeriodicalId\":19169,\"journal\":{\"name\":\"Neurological Research and Practice\",\"volume\":\" \",\"pages\":\"32\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9377119/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurological Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42466-022-00198-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-022-00198-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Single-center experience of induction therapy in non-systemic vasculitic neuropathy.
Background: No controlled studies for non-systemic vasculitic neuropathy treatment exist (NSVN). We compared the treatment response to induction therapy commonly used in clinical practice in NSVN.
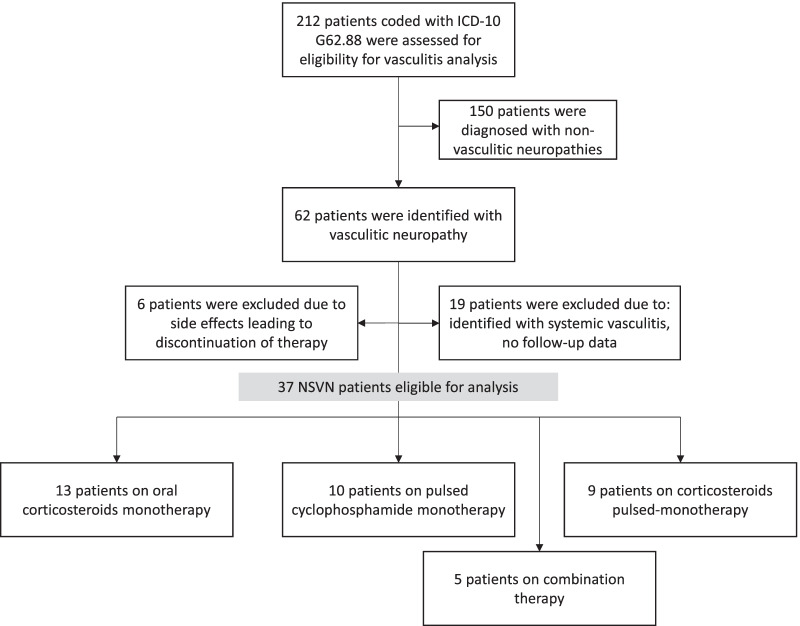
Methods: In this retrospective single-center study, 43 patients with biopsy-proven NSVN were analyzed. Patients were subdivided into groups depending on their initial treatment. Relapse rates, changes of motor and sensory symptoms, adverse events, predictors of relapses, and second-line treatment were compared.
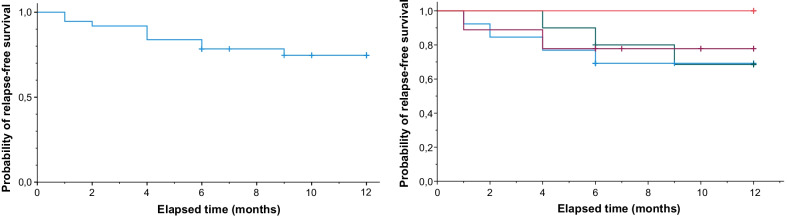
Results: Initial treatment regimens were corticosteroid monotherapy, cyclophosphamide monotherapy, pulsed corticosteroid therapy, and combination therapy. Discontinuation due to adverse events occurred in 6 of 43 patients. Clinical data did not differ between treatment groups. Within 12 months, 24.3% of patients relapsed. The median time to relapse was 4 (1.5, 6) months. No relapse occurred in the combination therapy group. However, there was no statistically significant difference in relapse-free survival between treatment groups (p = 0.58). Neither clinical data nor biopsy analysis predicted relapses sufficiently. As a second-line treatment, cyclophosphamide as mono- or combination therapy was used (7 of 9 patients) most frequently. One patient was treated with methotrexate, and one with IVIG.
Conclusions: Induction therapy used in clinical practice is effective and mainly well-tolerated in NSVN. Our data do not support an overall advantage of cyclophosphamide over corticosteroid monotherapy. Controlled trials comparing the effectiveness of induction and maintenance therapy in NSVN are warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


