Seoyeon Kim, Seondeuk Kim, Seonkyung Lee, Hyo-Jung Kim
{"title":"2型共济失调的垂直跳跃性减慢。","authors":"Seoyeon Kim, Seondeuk Kim, Seonkyung Lee, Hyo-Jung Kim","doi":"10.3988/jcn.2022.18.6.726","DOIUrl":null,"url":null,"abstract":"Dear Editor, Episodic ataxia (EA) is a group of disorders characterized by recurrent attacks of truncal ataxia and incoordination.1,2 Among the eight subtypes, EA type 2 (EA2) is the most common and is inherited in an autosomal dominant pattern due to mutations in the voltagegated Cav2.1 P/Q-type calcium channel (CACNA1A).2,3 Patients with EA2 typically present with recurrent ataxia that lasts minutes to hours with interictal ocular motor abnormalities mostly due to cerebellar dysfunction.1 Here we report vertical saccade slowing in a patient with EA2, which is a previously undescribed finding in this disorder. A 17-year-old man with a family history of EA2 had been followed up in a dizziness clinic for 7 years. His elder sister had a confirmed EA2 diagnosis based on characteristic clinical features and a heterozygous mutation (c.4953+1G>A) at the intron 31 splice donor site in the CACNA1A gene (reference sequence=NG_011569).4 Findings of the initial evaluation at 10 years old were conspicuous for gaze-evoked and downbeat nystagmus during lateral gaze (side-pocket nystagmus), and rebound upbeat nystagmus when resuming the straight-ahead gaze.4 There was a curved trajectory in the upward saccades, but the velocity was within the normal range.4 Smooth pursuit and visual enhancement of the vestibulo-ocular reflex were impaired in both the horizontal and vertical directions.4 The other findings of the patient and his family members have been described previously.4 A follow-up evaluation 7 years later additionally indicated slowing of the vertical saccades in both directions (Fig. 1; Supplementary Video 1 in the online-only Data Supplement). Horizontal saccades were normal (Fig. 1). Other findings of the neurological examination remained unchanged. Genetic analysis confirmed the same mutation as the one found in his sister. Our patient with EA2 due to a mutation in the CACNA1A gene presented with vertical saccade slowing during the follow-up at 7 years after the initial presentation. Premotor commands for saccades are generated in the brainstem via interactions between the burst and omnipause neurons.5 Disruption of these brainstem neural networks results in saccade slowing. The excitatory burst neurons for horizontal saccades lie in the paramedian pontine reticular formation, while those for vertical saccades reside in the rostral interstitial nucleus of the medial longitudinal fasciculus.5 In EA2, interictal ocular motor abnormalities have mostly been ascribed to cerebellar dysfunction and include downbeat nystagmus, gaze-evoked nystagmus, positional nystagmus, impaired smooth pursuit, and hypermetric saccades.2,6 However, the selective vertical saccade slowing observed in our patient with EA2 indicated an additional involvement of the upper midbrain in this disorder.7 It is interesting that previous reports also described slow horizontal saccades8 and internuclear ophthalmoparesis9 as rare findings in EA2, which also indicates a brainstem involvement in this disorder. Indeed, recent studies have found various phenotypes related to mutations that involve CACNA1A.10 Our report expands the clinical spectrum of EA2 and support extracerebellar involvements in this disorder. Seoyeon Kim Seondeuk Kim Seonkyung Lee Hyo-Jung Kim","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"726-728"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/17/jcn-18-726.PMC9669551.pdf","citationCount":"0","resultStr":"{\"title\":\"Vertical Saccadic Slowing in Episodic Ataxia Type 2.\",\"authors\":\"Seoyeon Kim, Seondeuk Kim, Seonkyung Lee, Hyo-Jung Kim\",\"doi\":\"10.3988/jcn.2022.18.6.726\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Episodic ataxia (EA) is a group of disorders characterized by recurrent attacks of truncal ataxia and incoordination.1,2 Among the eight subtypes, EA type 2 (EA2) is the most common and is inherited in an autosomal dominant pattern due to mutations in the voltagegated Cav2.1 P/Q-type calcium channel (CACNA1A).2,3 Patients with EA2 typically present with recurrent ataxia that lasts minutes to hours with interictal ocular motor abnormalities mostly due to cerebellar dysfunction.1 Here we report vertical saccade slowing in a patient with EA2, which is a previously undescribed finding in this disorder. A 17-year-old man with a family history of EA2 had been followed up in a dizziness clinic for 7 years. His elder sister had a confirmed EA2 diagnosis based on characteristic clinical features and a heterozygous mutation (c.4953+1G>A) at the intron 31 splice donor site in the CACNA1A gene (reference sequence=NG_011569).4 Findings of the initial evaluation at 10 years old were conspicuous for gaze-evoked and downbeat nystagmus during lateral gaze (side-pocket nystagmus), and rebound upbeat nystagmus when resuming the straight-ahead gaze.4 There was a curved trajectory in the upward saccades, but the velocity was within the normal range.4 Smooth pursuit and visual enhancement of the vestibulo-ocular reflex were impaired in both the horizontal and vertical directions.4 The other findings of the patient and his family members have been described previously.4 A follow-up evaluation 7 years later additionally indicated slowing of the vertical saccades in both directions (Fig. 1; Supplementary Video 1 in the online-only Data Supplement). Horizontal saccades were normal (Fig. 1). Other findings of the neurological examination remained unchanged. Genetic analysis confirmed the same mutation as the one found in his sister. Our patient with EA2 due to a mutation in the CACNA1A gene presented with vertical saccade slowing during the follow-up at 7 years after the initial presentation. Premotor commands for saccades are generated in the brainstem via interactions between the burst and omnipause neurons.5 Disruption of these brainstem neural networks results in saccade slowing. The excitatory burst neurons for horizontal saccades lie in the paramedian pontine reticular formation, while those for vertical saccades reside in the rostral interstitial nucleus of the medial longitudinal fasciculus.5 In EA2, interictal ocular motor abnormalities have mostly been ascribed to cerebellar dysfunction and include downbeat nystagmus, gaze-evoked nystagmus, positional nystagmus, impaired smooth pursuit, and hypermetric saccades.2,6 However, the selective vertical saccade slowing observed in our patient with EA2 indicated an additional involvement of the upper midbrain in this disorder.7 It is interesting that previous reports also described slow horizontal saccades8 and internuclear ophthalmoparesis9 as rare findings in EA2, which also indicates a brainstem involvement in this disorder. Indeed, recent studies have found various phenotypes related to mutations that involve CACNA1A.10 Our report expands the clinical spectrum of EA2 and support extracerebellar involvements in this disorder. Seoyeon Kim Seondeuk Kim Seonkyung Lee Hyo-Jung Kim\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"726-728\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/17/jcn-18-726.PMC9669551.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.6.726\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.6.726","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Vertical Saccadic Slowing in Episodic Ataxia Type 2.
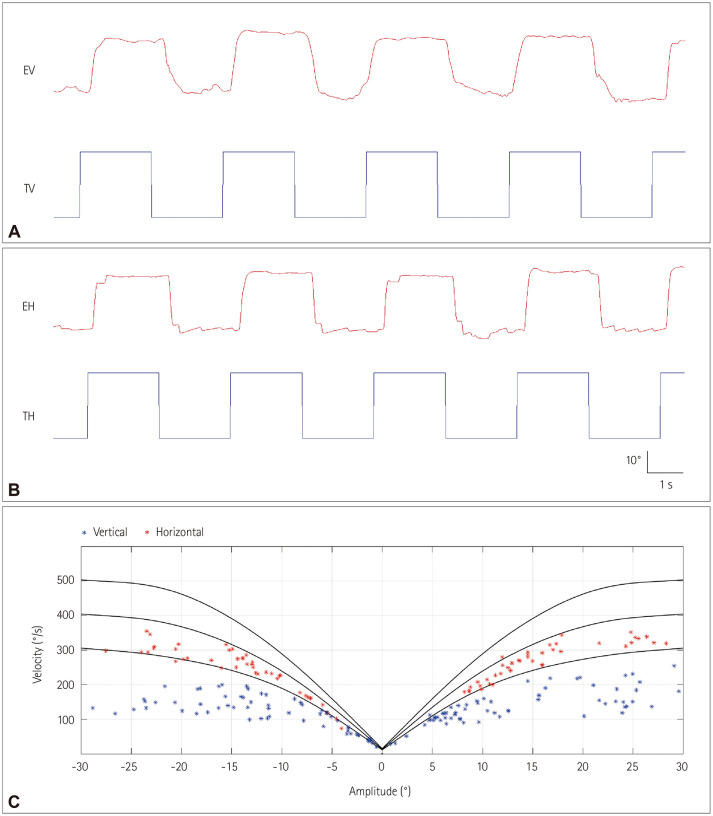
Dear Editor, Episodic ataxia (EA) is a group of disorders characterized by recurrent attacks of truncal ataxia and incoordination.1,2 Among the eight subtypes, EA type 2 (EA2) is the most common and is inherited in an autosomal dominant pattern due to mutations in the voltagegated Cav2.1 P/Q-type calcium channel (CACNA1A).2,3 Patients with EA2 typically present with recurrent ataxia that lasts minutes to hours with interictal ocular motor abnormalities mostly due to cerebellar dysfunction.1 Here we report vertical saccade slowing in a patient with EA2, which is a previously undescribed finding in this disorder. A 17-year-old man with a family history of EA2 had been followed up in a dizziness clinic for 7 years. His elder sister had a confirmed EA2 diagnosis based on characteristic clinical features and a heterozygous mutation (c.4953+1G>A) at the intron 31 splice donor site in the CACNA1A gene (reference sequence=NG_011569).4 Findings of the initial evaluation at 10 years old were conspicuous for gaze-evoked and downbeat nystagmus during lateral gaze (side-pocket nystagmus), and rebound upbeat nystagmus when resuming the straight-ahead gaze.4 There was a curved trajectory in the upward saccades, but the velocity was within the normal range.4 Smooth pursuit and visual enhancement of the vestibulo-ocular reflex were impaired in both the horizontal and vertical directions.4 The other findings of the patient and his family members have been described previously.4 A follow-up evaluation 7 years later additionally indicated slowing of the vertical saccades in both directions (Fig. 1; Supplementary Video 1 in the online-only Data Supplement). Horizontal saccades were normal (Fig. 1). Other findings of the neurological examination remained unchanged. Genetic analysis confirmed the same mutation as the one found in his sister. Our patient with EA2 due to a mutation in the CACNA1A gene presented with vertical saccade slowing during the follow-up at 7 years after the initial presentation. Premotor commands for saccades are generated in the brainstem via interactions between the burst and omnipause neurons.5 Disruption of these brainstem neural networks results in saccade slowing. The excitatory burst neurons for horizontal saccades lie in the paramedian pontine reticular formation, while those for vertical saccades reside in the rostral interstitial nucleus of the medial longitudinal fasciculus.5 In EA2, interictal ocular motor abnormalities have mostly been ascribed to cerebellar dysfunction and include downbeat nystagmus, gaze-evoked nystagmus, positional nystagmus, impaired smooth pursuit, and hypermetric saccades.2,6 However, the selective vertical saccade slowing observed in our patient with EA2 indicated an additional involvement of the upper midbrain in this disorder.7 It is interesting that previous reports also described slow horizontal saccades8 and internuclear ophthalmoparesis9 as rare findings in EA2, which also indicates a brainstem involvement in this disorder. Indeed, recent studies have found various phenotypes related to mutations that involve CACNA1A.10 Our report expands the clinical spectrum of EA2 and support extracerebellar involvements in this disorder. Seoyeon Kim Seondeuk Kim Seonkyung Lee Hyo-Jung Kim

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


