{"title":"偏头痛患者骨吸收标志物升高:一个病例系列。","authors":"Alberto Lerario","doi":"10.3988/jcn.2022.18.6.720","DOIUrl":null,"url":null,"abstract":"Dear Editor, Migraine is a debilitating headache characterized by pulsating quality, and is often on one side of the head and aggravated by movement. Excessive bone resorption due to osteoclast activity can lead to diminished bone strength. Although it may appear ambiguous, a recent study by Wu et al.1 suggested a pathophysiological link between osteoporosis and migraine. Magnesium and vitamin D levels are known to be vital for proper bone function, while they may regulate the frequency of migraines2 by shaping nociceptive processes in unmyelinated calcitonin gene-related peptide (CGRP)-positive neurons, a process also influenced by ovarian hormones.3 Inflammatory mediators such as certain interleukins and tumor necrosis factor-α contribute to endothelial dysfunction and pain pathways in migraine,4 and exerts a significant influence on bone turnover that induces osteoporosis. Moreover, inflammatory mediators play roles in activating the trigeminovascular system, which in turn releases proinflammatory substances, particularly CGRP. Elevated CGRP levels have also been found in subjects with osteoporosis and may indirectly regulate osteoclast activity.5 Furthermore, both of these diseases include high prevalence rates of migraine and osteoporosis in patients with inflammatory bowel disease,6 possibly due to multiple factors such as gut microbiota profile, stress hormones, nutrients, and neuropeptides that affect different intestinal bacterial strains.7 Finally, migraine causes social withdrawal with a consequent reduction in motor activity, and less exposure to light due to a reaction from photophobia. We present 19 patients with migraine who presented pathological bone turnover. In our private clinic, we evaluated 19 Italian adult patients (15 fertile females and 4 males) aged between 20 and 40 years over the course of 1 year. These patients were suffering from migraine with aura or migraine without aura according to the third edition of the International Classification of Headache Disorders (ICHD-3), or one or more migraine attacks per month for at least 6 months. All subjects did not show associated comorbidities or present a history of fragility fracture. All patients were not sedentary, followed a Mediterranean diet, and had body mass indices of 18.42–25.12 kg/m2 (Table 1). However, we did not further detail exercise capacity, smoking, or alcohol consumption in detail. None of the patients had taken prophylactic or contraceptive therapies within the past 5 years, and they utilized nonsteroidal anti-inflammatory drugs or triptans for symptomatic therapy. The sex, age, and migraine frequency distributions are listed in Table 1. The findings of physical and neurological examinations were unremarkable for all patients. Considering the frequent vitamin D deficiency in patients with migraine, we also performed bone profile laboratory tests. Serological tests were performed under fasting conditions and without taking into account the menstrual cycle for females. Complete blood count, calcium, phosphate, creatinine, alkaline phosphatase, aminotransferases, thyroid-stimulating hormone, and parathyroid hormone levels were within their respective normal ranges. Vitamin D deficiency or insufficiency (defined as <20, and ≥20 and <30 ng/mL 25[OH]D, reAlberto Lerario","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"720-722"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/be/da/jcn-18-720.PMC9669558.pdf","citationCount":"0","resultStr":"{\"title\":\"Elevated Bone Resorption Markers in Patients With Migraine: A Case Series.\",\"authors\":\"Alberto Lerario\",\"doi\":\"10.3988/jcn.2022.18.6.720\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Migraine is a debilitating headache characterized by pulsating quality, and is often on one side of the head and aggravated by movement. Excessive bone resorption due to osteoclast activity can lead to diminished bone strength. Although it may appear ambiguous, a recent study by Wu et al.1 suggested a pathophysiological link between osteoporosis and migraine. Magnesium and vitamin D levels are known to be vital for proper bone function, while they may regulate the frequency of migraines2 by shaping nociceptive processes in unmyelinated calcitonin gene-related peptide (CGRP)-positive neurons, a process also influenced by ovarian hormones.3 Inflammatory mediators such as certain interleukins and tumor necrosis factor-α contribute to endothelial dysfunction and pain pathways in migraine,4 and exerts a significant influence on bone turnover that induces osteoporosis. Moreover, inflammatory mediators play roles in activating the trigeminovascular system, which in turn releases proinflammatory substances, particularly CGRP. Elevated CGRP levels have also been found in subjects with osteoporosis and may indirectly regulate osteoclast activity.5 Furthermore, both of these diseases include high prevalence rates of migraine and osteoporosis in patients with inflammatory bowel disease,6 possibly due to multiple factors such as gut microbiota profile, stress hormones, nutrients, and neuropeptides that affect different intestinal bacterial strains.7 Finally, migraine causes social withdrawal with a consequent reduction in motor activity, and less exposure to light due to a reaction from photophobia. We present 19 patients with migraine who presented pathological bone turnover. In our private clinic, we evaluated 19 Italian adult patients (15 fertile females and 4 males) aged between 20 and 40 years over the course of 1 year. These patients were suffering from migraine with aura or migraine without aura according to the third edition of the International Classification of Headache Disorders (ICHD-3), or one or more migraine attacks per month for at least 6 months. All subjects did not show associated comorbidities or present a history of fragility fracture. All patients were not sedentary, followed a Mediterranean diet, and had body mass indices of 18.42–25.12 kg/m2 (Table 1). However, we did not further detail exercise capacity, smoking, or alcohol consumption in detail. None of the patients had taken prophylactic or contraceptive therapies within the past 5 years, and they utilized nonsteroidal anti-inflammatory drugs or triptans for symptomatic therapy. The sex, age, and migraine frequency distributions are listed in Table 1. The findings of physical and neurological examinations were unremarkable for all patients. Considering the frequent vitamin D deficiency in patients with migraine, we also performed bone profile laboratory tests. Serological tests were performed under fasting conditions and without taking into account the menstrual cycle for females. Complete blood count, calcium, phosphate, creatinine, alkaline phosphatase, aminotransferases, thyroid-stimulating hormone, and parathyroid hormone levels were within their respective normal ranges. Vitamin D deficiency or insufficiency (defined as <20, and ≥20 and <30 ng/mL 25[OH]D, reAlberto Lerario\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"720-722\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/be/da/jcn-18-720.PMC9669558.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.6.720\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.6.720","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Elevated Bone Resorption Markers in Patients With Migraine: A Case Series.
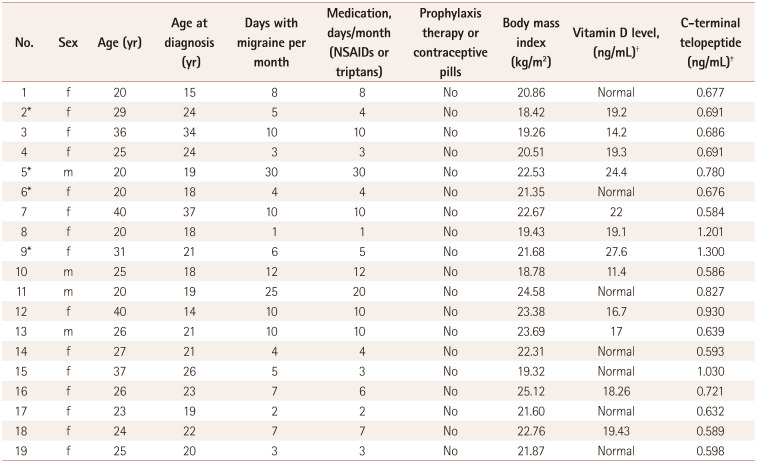
Dear Editor, Migraine is a debilitating headache characterized by pulsating quality, and is often on one side of the head and aggravated by movement. Excessive bone resorption due to osteoclast activity can lead to diminished bone strength. Although it may appear ambiguous, a recent study by Wu et al.1 suggested a pathophysiological link between osteoporosis and migraine. Magnesium and vitamin D levels are known to be vital for proper bone function, while they may regulate the frequency of migraines2 by shaping nociceptive processes in unmyelinated calcitonin gene-related peptide (CGRP)-positive neurons, a process also influenced by ovarian hormones.3 Inflammatory mediators such as certain interleukins and tumor necrosis factor-α contribute to endothelial dysfunction and pain pathways in migraine,4 and exerts a significant influence on bone turnover that induces osteoporosis. Moreover, inflammatory mediators play roles in activating the trigeminovascular system, which in turn releases proinflammatory substances, particularly CGRP. Elevated CGRP levels have also been found in subjects with osteoporosis and may indirectly regulate osteoclast activity.5 Furthermore, both of these diseases include high prevalence rates of migraine and osteoporosis in patients with inflammatory bowel disease,6 possibly due to multiple factors such as gut microbiota profile, stress hormones, nutrients, and neuropeptides that affect different intestinal bacterial strains.7 Finally, migraine causes social withdrawal with a consequent reduction in motor activity, and less exposure to light due to a reaction from photophobia. We present 19 patients with migraine who presented pathological bone turnover. In our private clinic, we evaluated 19 Italian adult patients (15 fertile females and 4 males) aged between 20 and 40 years over the course of 1 year. These patients were suffering from migraine with aura or migraine without aura according to the third edition of the International Classification of Headache Disorders (ICHD-3), or one or more migraine attacks per month for at least 6 months. All subjects did not show associated comorbidities or present a history of fragility fracture. All patients were not sedentary, followed a Mediterranean diet, and had body mass indices of 18.42–25.12 kg/m2 (Table 1). However, we did not further detail exercise capacity, smoking, or alcohol consumption in detail. None of the patients had taken prophylactic or contraceptive therapies within the past 5 years, and they utilized nonsteroidal anti-inflammatory drugs or triptans for symptomatic therapy. The sex, age, and migraine frequency distributions are listed in Table 1. The findings of physical and neurological examinations were unremarkable for all patients. Considering the frequent vitamin D deficiency in patients with migraine, we also performed bone profile laboratory tests. Serological tests were performed under fasting conditions and without taking into account the menstrual cycle for females. Complete blood count, calcium, phosphate, creatinine, alkaline phosphatase, aminotransferases, thyroid-stimulating hormone, and parathyroid hormone levels were within their respective normal ranges. Vitamin D deficiency or insufficiency (defined as <20, and ≥20 and <30 ng/mL 25[OH]D, reAlberto Lerario

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


